

ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗż(Vogt-Koyanagi-Harada)ļ│æņØĆ ņ¢æņĖĪņä▒ ņ£ĪņĢäņóģņä▒ ĒżļÅäļ¦ēņŚ╝ņØ┤ ĒŖ╣ņ¦ĢņĀüņØ┤ļ®░ ņןņĢĪņä▒ ļ¦Øļ¦ēļ░Ģļ”¼, ņŗ£ņŗĀĻ▓ĮļČĆņóģĻ│╝ Ļ░ÖņØĆ ņĢłĻ│╝ņĀü ņ”ØņāüĻ│╝ ļŹöļČłņ¢┤ ļæÉĒåĄ, ņØ┤ļ¬ģ ļō▒ņØś ņŗĀĻ▓ĮĒĢÖņĀü ņ”Øņāü ļśÉĒĢ£ ļÅÖļ░śļÉĀ ņłś ņ׳ļŖö ņ×ÉĻ░Ćļ®┤ņŚŁņä▒ ņ¦łĒÖśņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. Ēśäņ×¼ ļ░ØĒśĆņ¦ä ņŻ╝ļÉ£ ļ│æĒā£ņāØļ”¼ļŖö ļ¦źļØĮļ¦ē ļō▒ ņĀäņŗĀņØś ļ®£ļØ╝ļŗīņäĖĒżļź╝ Ēæ£ņĀüņ£╝ļĪ£ ĒĢśļŖö CD4+ TņäĖĒż ļ¦żĻ░£ ļ®┤ņŚŁļ░śņØæņØ┤ļ®░ ņØ┤ Ļ│╝ņĀĢņŚÉņä£ ņŚ¼ļ¤¼ ņé¼ņØ┤ĒåĀņ╣┤ņØĖļōżņØ┤ ņśüĒ¢źņØä ļ»Ėņ╣śļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.1
ņĮöļĪ£ļéśļ░öņØ┤ļ¤¼ņŖżĻ░ÉņŚ╝ņ”Ø-19 (COVID-19)ļŖö SARS-CoV-2 ļ░öņØ┤ļ¤¼ņŖżņŚÉ ņØśĒĢ£ ĻĖēņä▒ ĒśĖĒØĪĻĖ░ ņĀäņŚ╝ļ│æņ£╝ļĪ£ ņĀäņäĖĻ│äņĀü ņ£ĀĒ¢ēņŚÉ ļö░ļØ╝ ņŚ¼ļ¤¼ ļ░▒ņŗĀļōżņØ┤ Ļ░£ļ░£ļÉśņŚłĻ│Ā ļ░▒ņŗĀņØś ņŚ¼ļ¤¼ ļČĆņ×æņÜ®ļōż ņżæ ņĢłĻ│╝ņĀüņ£╝ļĪ£ļŖö ĒżļÅäļ¦ēņŚ╝, ļ¦Øļ¦ēņĀĢļ¦źĒÅÉņćä, ņżæņŗ¼ņןņĢĪļ¦źļØĮļ¦Øļ¦ēļ│æņ”Ø, ĻĖēņä▒ ĒÖ®ļ░śņŗĀĻ▓Įļ¦Øļ¦ēļ│æņ”Ø ļō▒ņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŗż.2 ĻĘĖņżæ ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņŚÉ ļīĆĒĢ£ ļ│┤Ļ│ĀļŖö ņāüļīĆņĀüņ£╝ļĪ£ ļō£ļ¼Ė ņāüĒā£ļĪ£ ĻĄŁļé┤ņŚÉņä£ļŖö mRNA-1273 ļ░▒ņŗĀ(Moderna, Cambridge, MA, USA) ņØ┤Ēøä ļ░£ņāØĒĢ£ ņ”ØļĪĆļ¦īņØ┤ ļ░£Ēæ£ļÉśņŚłļŗż.3 ņØ┤ņŚÉ ņĀĆņ×ÉļōżņØĆ ĻĄŁļé┤ņŚÉņä£ BNT162b2 ļ░▒ņŗĀ(Comirnaty, Pfizer-BioNTech, New York, NY, USA) ņĀæņóģ ņØ┤Ēøä ļ░£ņāØĒĢ£ ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æ 1ņśłļź╝ ņĄ£ņ┤ł ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”ØļĪĆļ│┤Ļ│Ā
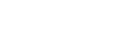
53ņäĖ ņŚ¼ņ×ÉĻ░Ć COVID-19 ļ░▒ņŗĀ(Pfizer-BioNTech) 3ņ░© ņĀæņóģĒĢ£ ļŗ¼ ĒøäļČĆĒä░ ņŗ£ņ×æļÉ£ ņ¢æņĢłņØś ņŗ£ļĀźņĀĆĒĢś, ņČ®Ēśł, ņĢłĻĄ¼ĒåĄņ”Ø ļ░Å ļæÉĒåĄņØä ņŻ╝ņåīļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. Ļ│Āņ¦ĆĒśłņ”Ø ņÖĖ ĒŖ╣ņØ┤ ļé┤Ļ│╝ņĀü ņ¦łĒÖśņØś Ļ│╝Ļ▒░ļĀźņØĆ ņŚåņŚłņ£╝ļ®░ ņĢłĻ│╝ņĀü ĒŖ╣ņØ┤ ļ│æļĀź ļśÉĒĢ£ ņŚåļŖö ĒÖśņ×ÉņśĆļŗż. ņ”Øņāü ļ░£Ēśä 1ņŻ╝ņØ╝ Ēøä ļ│ĖņøÉ ņ┤łņ¦ä ļŗ╣ņŗ£ ļéśņĢłņŗ£ļĀź(Snellen) ņ¢æņĢł 0.5 ļ░Å Ēśäņä▒ĻĄ┤ņĀłĻ▓Ćņé¼ņŚÉ ņØśĒĢ£ ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀź ņÜ░ņĢł 0.63, ņóīņĢł 1.0ņØ┤ņŚłņ£╝ļ®░, ļ╣äņĀæņ┤ē ņĢłņĢĢĻ│äļĪ£ ņĖĪņĀĢĒĢ£ ņĢłņĢĢņØĆ ņÜ░ņĢł 19 mmHg, ņóīņĢł 21 mmHgņśĆļŗż. ņäĖĻĘ╣ļō▒Ļ▓Ćņé¼ņāü ņ¢æņĢłņŚÉ ņĀäļ░®ņŚ╝ņ”Ø 2+ ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā ņĢłņĀĆĻ▓Ćņé¼ ļ░Å ļ╣øĻ░äņäŁļŗ©ņĖĄĻ▓Ćņé¼ņāü ņ¢æņĢł ņŗ£ņŗĀĻ▓Įņ£ĀļæÉļČĆņóģ, ļ¦źļØĮļ¦ē ņĀæĒל, ļŗżļ░£ņØś ĻĄŁņåīņĀü ņןņĢĪņä▒ ļ¦Øļ¦ēļ░Ģļ”¼, ĒśĢĻ┤æņĢłņĀĆĒśłĻ┤ĆņĪ░ņśüņłĀņāü ņ¢æņĢł ĒøäĻĘ╣ļČĆ ņĪ░ņśüņĀ£ ļłäņČ£ ļśÉĒĢ£ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 1). ņØ┤ņŚÉ ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņ£╝ļĪ£ ņ¦äļŗ©ĒĢś 0.5% levofloxacin (Cravit, Santen Pharmaceutical, Osaka, Japan)Ļ│╝ 1% prednisolone acetate (Predforte┬«, Allergan Inc., Irvine, CA, USA)ļź╝ ņ¢æņĢł 4ņŗ£Ļ░äļ¦łļŗż ņĀÉņĢł ļ░Å Ļ▓ĮĻĄ¼ prednisolone (Solondo, Yuhan Corporation, Seoul, Korea) ĒĢśļŻ© 30 mgņö® 2ņ░©ļĪĆ, ņ┤Ø 60 mg ļ│ĄņÜ®ņ£╝ļĪ£ ņ╣śļŻīļź╝ ņŗ£ņ×æĒĢśņśĆļŗż.
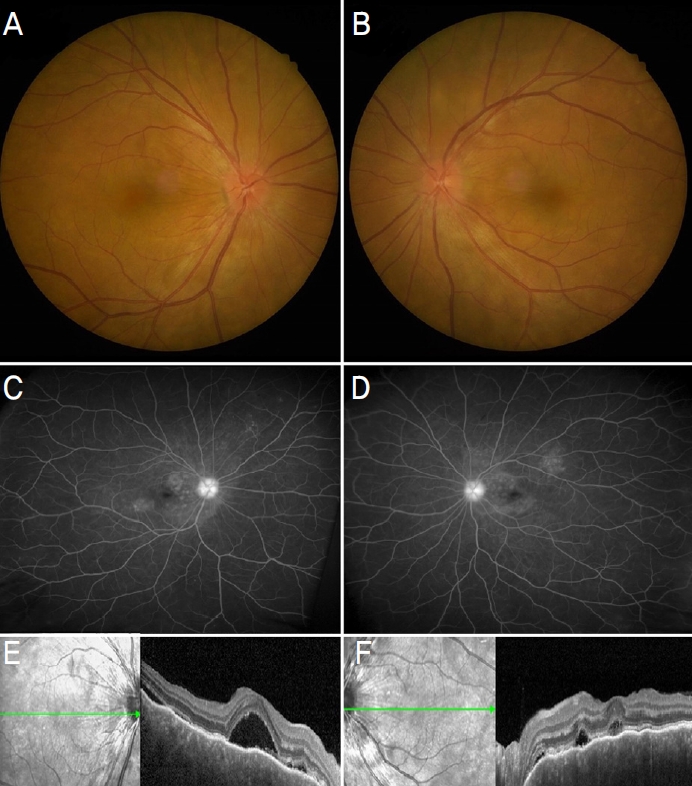
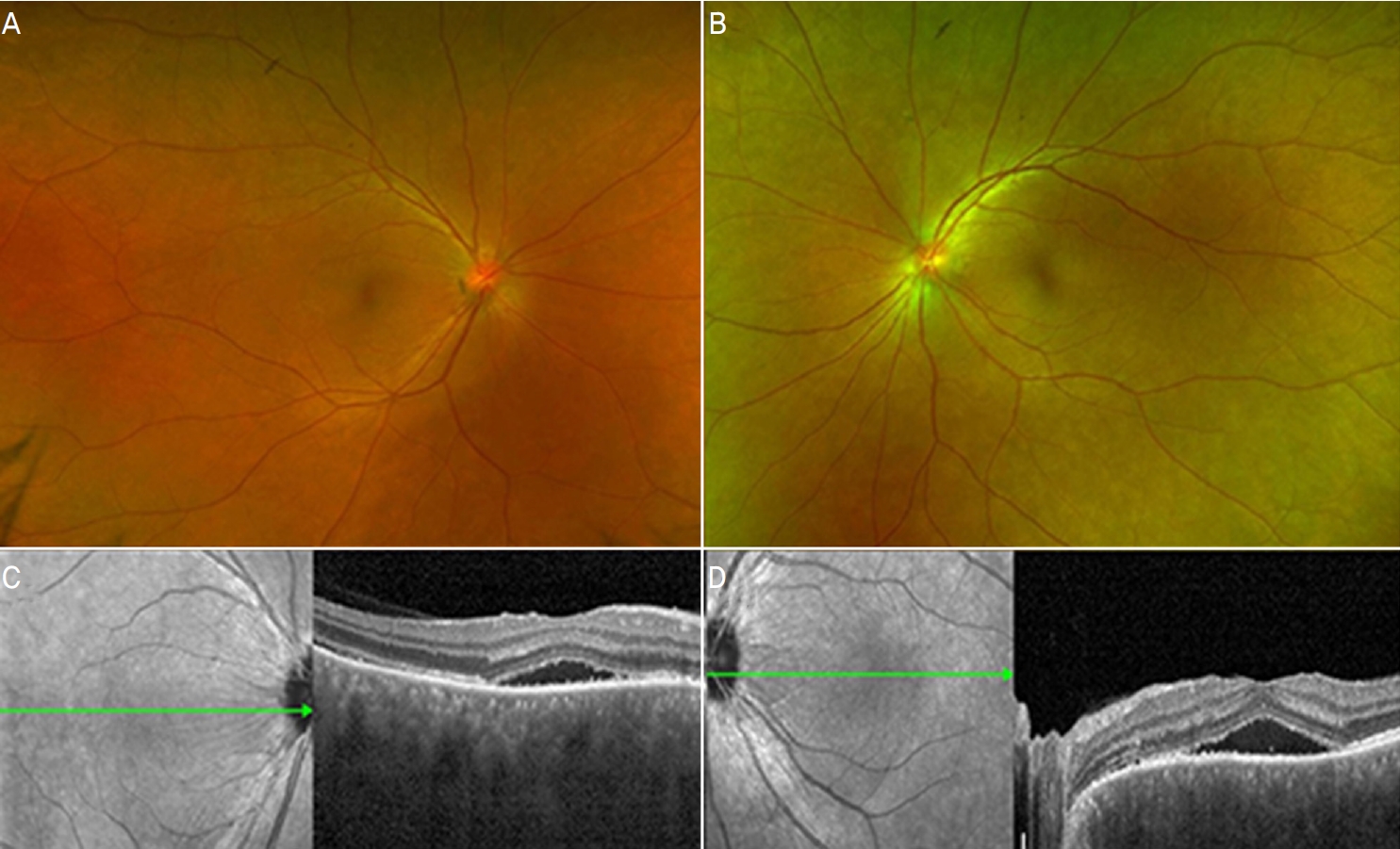
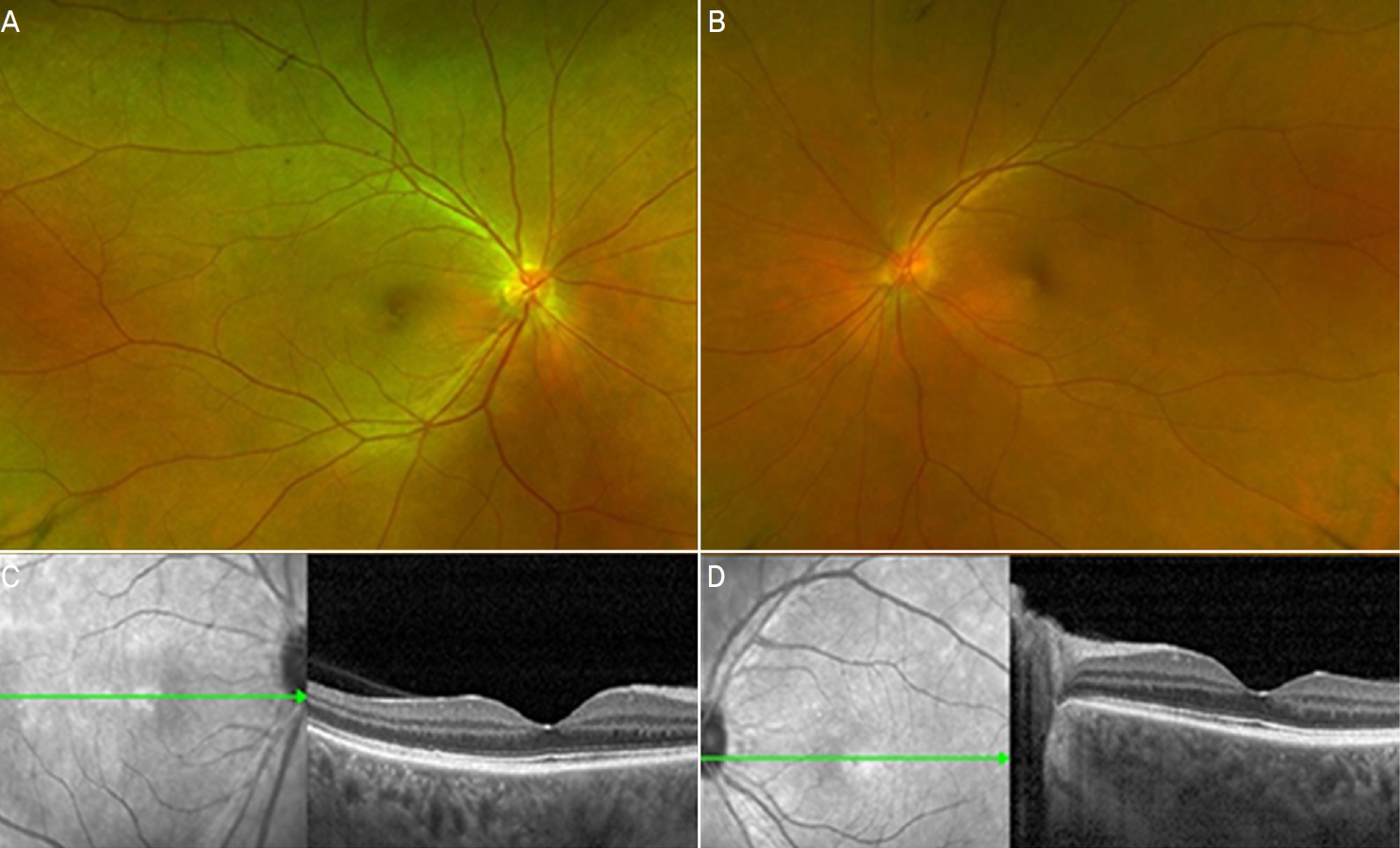
1ņŻ╝ņØ╝ Ēøä ļé┤ņøÉĒĢ£ ņÖĖļלņŚÉņä£ ļéśņĢłņŗ£ļĀźņØĆ ņÜ░ņĢł 0.3, ņóīņĢł 0.15ļĪ£ ļŗżņåī Ļ░ÉņåīĒĢ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆņ£╝ļéś ņ¢æņĢł ņĢłĻĄ¼ĒåĄņ”Ø ļ░Å ņŗ£ņĢ╝ĒØÉļ”╝ņŚÉ ļīĆĒĢ£ ņŻ╝Ļ┤ĆņĀü ņ”ØņāüņØĆ ļ¦ÄņØ┤ ĒśĖņĀäļÉ£ ņāüĒā£ņśĆĻ│Ā ņäĖĻĘ╣ļō▒Ļ▓Ćņé¼ņŚÉņä£ ņĀäļ░®ņŚ╝ņ”ØņØĆ Ļ▒░ņØś Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ļśÉĒĢ£ ņĢłņĀĆ Ļ▓Ćņé¼ ļ░Å ļ╣øĻ░äņäŁļŗ©ņĖĄĻ▓Ćņé¼ ņāüņ£╝ļĪ£ļÅä ņ¢æņĢł ļ¬©ļæÉ ņןņĢĪļ¦Øļ¦ēļ░Ģļ”¼ Ļ░Éņåī ņåīĻ▓¼ņØä ļ│┤ņŚ¼ ņĢłņĢĮ ĒĢśļŻ© 4ļ▓ł ļ░Å Ļ▓ĮĻĄ¼ ņĢĮņĀ£ 1ņŻ╝ Ļ░äĻ▓®ņ£╝ļĪ£ 10 mgņö® Ļ░Éļ¤ēĒĢśļ®░ Ļ▓ĮĻ│╝ļź╝ ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 2). Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£ 2Ļ░£ņøö Ēøä ļé┤ņøÉĒĢ£ ņÖĖļלņŚÉņä£ ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀź ņ¢æņĢł 1.0ņ£╝ļĪ£ ņĖĪņĀĢļÉśņŚłĻ│Ā ņĀäļ░®ņŚ╝ņ”Ø ņŚåņØ┤ ņ¢æņĢł ļ¦Øļ¦ēņØ┤ ņÖäņĀäĒ׳ ņĀĢņāüĒÖöļÉ£ Ļ▓āņØ┤ ĒÖĢņØĖļÉśņ¢┤ ļ¬©ļōĀ ņĢĮņØä ņżæļŗ©ĒĢśņśĆņ£╝ļ®░ ĻĘĖļĪ£ļČĆĒä░ 3Ļ░£ņøö ĒøäņØĖ ļ¦łņ¦Ćļ¦ē ņÖĖļלņŚÉņä£ ĒÖĢņØĖĒĢ£ Ļ▓Ćņé¼ ņāüņ£╝ļĪ£ļÅä ņ×¼ļ░£ņØĆ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 3).
Ļ│Ā ņ░░
ļ│Ė ņ”ØļĪĆļŖö ĒŖ╣ņØ┤ ņĢłĻ│╝ņĀü ļ│æļĀź ļ░Å ņłśņłĀļĀź ņŚåļŖö ĒÖśņ×ÉņŚÉņä£ BNT162b2 ļ░▒ņŗĀ ņĀæņóģ ĒĢ£ ļŗ¼ Ēøä ļ░£ņāØĒĢ£ ļæÉĒåĄ, ņ¢æņĢłņØś ņŗ£ļĀźņĀĆĒĢś, ņĀäļ░®ņŚ╝ņ”Ø, ņןņĢĪņä▒ ļ¦Øļ¦ēļ░Ģļ”¼, ņŗ£ņŗĀĻ▓ĮļČĆņóģ ļ░Å ļ¦źļØĮļ¦ēņŚ╝ ņåīĻ▓¼ņ£╝ļĪ£ ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ Ļ▓ĮņÜ░ņØ┤ļŗż. ņŗżņĀ£ ĒĢ┤ņÖĖ ļģ╝ļ¼ĖņØä ĒåĄĒĢ┤ ļ│┤Ļ│ĀļÉ£ COVID-19 ļ░▒ņŗĀ ņĀæņóģ Ēøä ņĢłĻ│╝ņĀü ņØ┤ņāü ļ░śņØæļōżņØä ņé┤ĒÄ┤ļ│┤ļ®┤ ņłśņØ╝ņŚÉņä£ ņłśņŻ╝Ļ╣īņ¦Ć ļŗżņ¢æĒĢ£ ĒśĢĒā£ļĪ£ ļČĆņ×æņÜ®ņØ┤ ļ░£ņāØĒĢ£ Ļ▓āņØä ņĢī ņłś ņ׳ņ£╝ļ®░ ņżæņ”ØņØś Ļ▓ĮņÜ░ ĒżļÅäļ¦ēņŚ╝ņØ┤ Ļ░Ćņן ĒØöĒĢśņśĆĻ│Ā ĻĘĖ ļ░¢ņŚÉļÅä ņŗ£ņŗĀĻ▓ĮņŚ╝, ļ¦Øļ¦ēĒśłĻ┤Ć ņ¦łĒÖś ļō▒ņØ┤ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż.2,4
ĻĘĖņżæ ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņŚÉ ļīĆĒĢ£ ņ”ØļĪĆļŖö ļŗżņä» ņśłĻ░Ć ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░ ĻĄŁļé┤ņŚÉņä£ļŖö mRNA-1273 ļ░▒ņŗĀ ņĀæņóģ ņØ┤Ēøä ļ░£ņāØĒĢ£ ĒÖśņ×ÉņŚÉ ļīĆĒĢ£ ĒĢ┤ņÖĖ ļģ╝ļ¼Ėļ¦īņØ┤ ņĪ┤ņ×¼ĒĢ£ļŗż.3,5-8 ĒŖ╣ņØ┤ Ļ│╝Ļ▒░ļĀź ņŚåļŹś 50ņäĖ ņŚ¼ĒÖśņØ┤ ņ▓½ ļ░▒ņŗĀ ņĀæņóģ 35ņØ╝ ņØ┤Ēøä ļ░£ņāØĒĢ£ ņ¢æņĢłņØś ņŗ£ļĀźņĀĆĒĢś, ņĢłĻĄ¼ĒåĄ, ļæÉĒåĄņ£╝ļĪ£ ļé┤ņøÉĒĢś ņ¦äļŗ©ļÉ£ Ļ▓ĮņÜ░ļĪ£ mRNA-1273 ļ░▒ņŗĀņØĆ ļ│Ė ņ”ØļĪĆņØś BNT162b2 ļ░▒ņŗĀĻ│╝ ņ£Āņé¼ĒĢ£ ļ░®ņŗØņØś mRNA ļ░▒ņŗĀņØ┤ļØ╝ļŖö ņĀÉņŚÉņä£ ņ£ĀņØśļ»ĖĒĢ£ Ļ┤ĆĻ│äĻ░Ć ņ׳ļŗżĻ│Ā ĒīÉļŗ©ļÉ£ļŗż.3 ņØ┤ ļ░¢ņŚÉļÅä ļÅÖņØ╝ĒĢ£ BNT162b2 ļ░Å ņĢäļŹ░ļģĖļ░öņØ┤ļ¤¼ņŖż ļ▓ĪĒä░ ļ░▒ņŗĀņØĖ AZD1222 (Oxford/AstraZeneca) ļō▒ ļŗżņ¢æĒĢ£ ņóģļźśņØś ļ░▒ņŗĀņŚÉ ļīĆĒĢ┤ņä£ļÅä ļ╣äņŖĘĒĢ£ ņ”ØļĪĆļōżņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŗż.5-7 ļśÉĒĢ£ ļ░▒ņŗĀ ņĀæņóģ ņÖĖņŚÉļÅä ņŗżņĀ£ COVID-19 Ļ░ÉņŚ╝ Ēøä ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņ£╝ļĪ£ ņ▓½ ņ¦äļŗ©ļÉ£ Ļ▓ĮņÜ░ļÅä ņ׳ņŚłļŗż.9,10 Ēśäņ×¼Ļ╣īņ¦Ć mRNA ļ░▒ņŗĀ Ēł¼ņŚ¼Ļ░Ć ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņØä ņ£Āļ░£ĒĢśļŖö ņĀĢĒÖĢĒĢ£ ĻĖ░ņĀäņØĆ ņĢīļĀżņ¦ä ļ░öĻ░Ć ņŚåņ£╝ļéś, Ļ░ĆļŖźĒĢ£ ļ░£ņāØ ĻĖ░ņĀäņ£╝ļĪ£ļŖö ņÜ░ņäĀ mRNA ņĀäļŗ¼ Ļ│╝ņĀĢņŚÉņä£ ļČäņ×ÉņĀü ņ£Āņé¼ņä▒ņ£╝ļĪ£ Ļ┤ĆļĀ©ļÉ£ ņé¼ņØ┤ĒåĀņ╣┤ņØĖņØ┤ ĒÖ£ņä▒ĒÖöļÉśņ¢┤ ņ×ÉĻ░Ćļ®┤ņŚŁ ļ░śņØæņØä ņ£Āļ░£ĒĢśņśĆņØä ņłś ņ׳ļŗż.11 ļśÉĒĢ£, RNA ļ░▒ņŗĀņØś ņ¦Ćņ¦łļéśļģĖņ×ģņ×É(mRNA-containing lipid nanoparticles) ļśÉļŖö ļ®┤ņŚŁņ”ØĻ░ĢņĀ£(adjuvant)Ļ░Ć ļ®┤ņŚŁļ░śņØæņØä ĒĢŁņ¦äņŗ£ņ╝£ ļ®┤ņŚŁĒĢÖņĀü ļČłĻĘĀĒśĢņØä Ļ░ĆņĀĖņÖöņØä ņłś ņ׳ļŗż.12 Ēśäņ×¼Ļ╣īņ¦ĆļŖö ļ░▒ņŗĀ Ēł¼ņŚ¼Ļ░Ć ĻĖ░ņ¦łņĀüņ£╝ļĪ£ ņåīņØĖņØ┤ ņ׳ņ¢┤ Ļ▓░ĻĄŁ ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņØ┤ ļ░£ĒśäļÉĀ ĒÖśņ×ÉņŚÉņä£ ļ░£ļ│æņØä ņĢ×ļŗ╣ĻĖ░ļŖö Ļ▓āņØĖņ¦Ć ņĀĢĒÖĢĒ׳ ņĢīĻĖ░ ņ¢┤ļĀĄļŗż. ļ│┤ĻĘĖĒŖĖ-Ļ│ĀņĢ╝ļéśĻĖ░-ĒĢśļØ╝ļŗżļ│æņØś ņŻ╝ļÉ£ ļ│æĒā£ņāØļ”¼ļŖö CD4+ TņäĖĒż ļ¦żĻ░£ ļ®┤ņŚŁļ░śņØæņØ┤ļ®░ ĒŖ╣Ē׳ TņäĖĒżļŖö interleukin (IL)-17, IL-23 ļō▒ņØś ņé¼ņØ┤ĒåĀņ╣┤ņØĖņØä ĒåĄĒĢ┤ ņŚ╝ņ”Øļ░śņØæņØä ņØ╝ņ£╝Ēé©ļŗżĻ│Ā ņĢīļĀżņĀĖ ņ׳ļŖöļŹ░ ņ×äņāü ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ COVID-19 mRNA ļ░▒ņŗĀ ņĀæņóģ Ēøä ļ╣äņŖĘĒĢ£ ĻĖ░ņĀäņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗżļŖö Ļ▓āņØ┤ ļ░ØĒśĆņĪīļŗż.1,13-15
ņØ┤ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ļÅÖņØ╝ ļ░▒ņŗĀņØś 3ņ░© ņĀæņóģņØ┤ņŚłļŗżļŖö ņĀÉ, ņĀæņóģĒĢ£ ļŗ¼ Ēøä ņ”ØņāüņØ┤ ļ░£ņāØĒĢśņśĆļŗżļŖö ņĀÉņŚÉņä£ ĒÖĢņŗżĒĢ£ ņŚ░Ļ┤Ćņä▒ņØĆ ļČĆņĪ▒ĒĢĀ ņłś ņ׳ļŗż. ņĄ£ĻĘ╝ ļ░£Ēæ£ļÉ£ COVID-19 ļ░▒ņŗĀ Ļ┤ĆļĀ© ĒżļÅäļ¦ēņŚ╝ ĒÖśņ×ÉļōżņØś ļīĆĻĘ£ļ¬© ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ ņØ┤ņāüļ░śņØæņØĆ ļīĆĻ░£ 1ņ░© ņĀæņóģ Ēøä, 1ņŻ╝ ņØ┤ļé┤ ļ░£ņāØĒĢśņśĆļŗżļŖö ļ│┤Ļ│ĀĻ░Ć ņ׳ļŗż.16 ĒĢśņ¦Ćļ¦ī COVID-19 ļ░▒ņŗĀ Ēøä ļ░£ņāØĒĢ£ ĻĄŁļé┤ ņżæņČöņŗĀĻ▓ĮĻ│ä ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖś ļ│┤Ļ│ĀņŚÉņä£ ļ░▒ņŗĀņØś ņł£ņä£ļŖö ņ”Øņāü ļ░£ĒśäņŚÉ Ēü░ ņŚ░Ļ┤ĆņØ┤ ņŚåņØīņØä ļ│┤Ļ│ĀĒĢ£ ļ░ö ņ׳Ļ│Ā ļ░▒ņŗĀ Ēł¼ņŚ¼ņÖĆ ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖś ļ░£ņāØ ņé¼ņØ┤ ņŚ░Ļ┤Ćņä▒ņŚÉ ļīĆĒĢ£ ņĀĢĒÖĢĒĢ£ ņŗ£Ļ░äņĀü ĻĖ░ņżĆņØ┤ ņŚåļŖö ņāüĒā£ņŚÉņä£ ļŗżļźĖ ņ£Āļ░£ ņÜöņØĖņØ┤ ņŚåļŖö ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ļ░▒ņŗĀ ņ£Āļ░£ Ļ░ĆļŖźņä▒ņØä ņÜ░ņäĀņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢ┤ ļ│╝ ņłś ņ׳ļŗż.17 ļśÉĒĢ£ ļ│Ė ņ”ØļĪĆļź╝ ĒżĒĢ©ĒĢśņŚ¼ ļīĆļŗżņłśņØś ĒÖśņ×ÉņŚÉņä£ Ļ▓ĮĻĄ¼ ņŖżĒģīļĪ£ņØ┤ļō£ ļ░Å ņĢłņĢĮ ņ╣śļŻīļ¦īņ£╝ļĪ£ļÅä ĒśĖņĀäļÉśņŚłĻ│Ā ļīĆĻĘ£ļ¬© ņŚ░ĻĄ¼ ņāüņ£╝ļĪ£ļÅä ļ░▒ņŗĀ ņĀæņóģ Ļ┤ĆļĀ© ĒżļÅäļ¦ēņŚ╝ņØś ļ╣äņ£©ņØ┤ ĒśäņĀĆĒ׳ ļé«ņĢä ņĀæņóģ ņŗ£ ņĢłĻ│╝ņĀü ļČĆņ×æņÜ®ņŚÉ ļīĆĒĢ£ ņČ®ļČäĒĢ£ ņäżļ¬ģņØä ĒåĄĒĢ┤ ļ╣ĀļźĖ ņ╣śļŻīĻ░Ć ņØ┤ļŻ©ņ¢┤ņ¦ł Ļ▓ĮņÜ░, ļ│┤ļŗż ņĢłņĀäĒĢ£ ļ░▒ņŗĀ ņĀæņóģņØ┤ Ļ░ĆļŖźĒĢĀ Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż.16

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






