

국민건강보험공단의 2021년 주요수술통계 연보에 따르면 국내 전체 의료기관에서 가장 많이 이뤄진 수술은 백내장수술로 1년간 약 78만건이 진행되었다.1 다초점 및 난시 교정 인공수정체의 발전 및 보편화에 따라 백내장수술은 잔여 굴절력을 줄임으로써 최대 나안시력을 얻는 것을 목표로 발전하고 있다. 백내장 환자들의 술 후 나안시력은 인공수정체 도수 계산에 의해 결정되며 사용되는 공식마다 요구하는 변수에 다소 차이는 있으나 각막굴절력 및 안축장이 주요 변수로 작용한다.2
지금까지는 주로 표준 각막곡률값(standard keratometry, K)을 사용하여 인공수정체 도수를 계산하였으며 이때 각막 후면은 정해진 굴절률인 1.3375를 대입하여 계산하였다. 그러나 각막의 총 곡률값은 각막 전면 곡률(anterior corneal curvature) 및 각막 후면 곡률(posterior corneal curvature), 각막두께에 의해 결정되며 각막 후면 곡률을 고려하지 않을 경우 정확한 각막 총 곡률값 및 난시 추정이 불가함을 여러 논문들에서 발표하였다.3-7 총 각막곡률값(total keratometry, TK)은 각막의 전면과 더불어 각막 후면 곡률 및 각막두께를 포함한 곡률값으로 특히 도난시 혹은 사난시 환자, 과거 각막굴절교정수술을 받은 환자에서 인공수정체 도수 계산에 유용한 것으로 알려져있으며,3,6,8-10 Barrett TK Universal II와 같이 총 각막곡률값을 기반으로 개발된 공식이 사용되고 있다.
각막 후면을 측정하기 위해 여러 장비들이 개발되었는데, 먼저 IOL Master 700® (Carl Zeiss Meditech AG, Jena, Germany)은 텔레센트릭(telecentric) 각막곡률 측정 방식과 파장가변 빛간섭단층촬영 방식을 사용하여 각막 전면과 후면, 안축장 등을 포함하는 전안부 계측 및 인공수정체 도수 계산이 가능하도록 고안되었다.11 Pentacam HR® (OCULUS, Wetzlar, Germany)은 샤임플러그 카메라 방식의 세극등 원리를 이용하여 각막 형태를 분석하고 각막 전면과 후면의 고위 수차를 산출 가능한 각막지형도 검사기이다.12 최근 새롭게 도입된 파장가변 빛간섭단층촬영계인 Anterion® (Heidelberg Engineering Inc., Heidelberg, Germany)은 1,300-nm wave-length swept laser를 이용하여 3차원 상을 만들어낸다.13 IOL Master와 측정 방식이 동일하며 두 기기와 마찬가지로 각막 후면 값을 측정할 수 있다.
각막은 전체 굴절력의 약 2/3를 차지하므로 최적의 굴절 결과를 얻기 위해서는 각막의 두께, 곡률 및 난시의 정확한 계측이 중요하다. 2017년 발간된 논문에서 IOL Master 500®, IOL Master 700®, Pentacam HR®을 이용하여 각막곡률, 안축장, 전방깊이 비교 시 세 기기 간 통계적으로 유의한 차이를 보이지 않았다고 보고되었으며,14 2022년 IOL Master 700®과 Anterion® 간의 인공수정체 도수 계산 비교 연구에서 두 장비 간 차이가 없음이 보고된 바 있다.15 본 연구에서 저자들은 Anterion®과 Pentacam HR®으로 측정한 여러 각막계측치 간 일치도를 비교하여, 새로 개발된 파장 가변 빛간섭단층촬영계인 Anterion®의 정확성 및 임상적 유용성을 알아보고자 하였다.
대상과 방법
2022년 1월 17일부터 2022년 2월 3일까지 가톨릭대학교 여의도성모병원 안과 외래에 내원한 환자 중 Anterion®과 Pentacam HR®을 모두 시행한 20명 26안, 2023월 5월 1일부터 2023년 5월 22일까지 가톨릭대학교 서울성모병원 안과 외래에 내원한 환자 중 Anterion®과 Pentacam HR®을 모두 시행한 23명 39안의 의무기록을 후향적으로 분석하였다. 본 연구는 가톨릭대학교 여의도성모병원 임상연구심의위원회(Institutional Review Board [IRB]; SC22RASI0210) 및 서울성모병원 임상연구심의위원회(IRB; KC23RADI0445)의 승인을 받아 진행하였고 헬싱키선언(Declaration of Helsinki)을 준수하였다.
모든 환자들은 시력 및 안압 측정, 현성굴절검사, 세극등현미경검사를 시행하였고, Anterion®과 Pentacam HR®은 2명의 검사자에 의해 시행되었다. 턱과 이마를 받침대에 고정한 상태에서 움직이지 않도록 하였고, 눈물막의 영향을 최소화하기 위해 검사 전 눈을 깜빡이게 하여 눈물층을 균일하게 하였으며 검사자에 의해 안구가 눌리지 않도록 주의하며 검사를 시행하였다. “Poor aquisition quality”로 확인되는 경우는 연구 대상에서 제외하였다.
각막 전면 및 후면의 가파른 축의 곡률(steep K [diopters, D]), 편평한 축의 곡률(flat K [D]) 및 평균 곡률(mean K [D])를 측정하였고, 난시벡터분석을 통해 잭슨교차원주(Jackson cross-cylinder, JCC) 값인 카티지언 난시(Cartesian astigmatism, J0) 및 경사난시(oblique astigmatism, J45)를 평가하였다. J0는 90°와 180° 난시축을 이용한 값으로 음성(negative)일 경우 도난시(against-the-rule astigmatism)를, 양성(positive)일 경우 직난시(with-the-rule astigmatism)를 의미하며, J45는 45°와 135° 난시축을 이용한 값으로 경사 난시를 의미하고 J0 및 J45는 다음과 같은 식으로 구하였다: J0=(-C/2) cos (2α), J45=(-C/2) sin (2α), (C=cylinder; α =axis).
또한, 전방깊이(anterior chamber depth, ACD [mm])와 중심각막두께(central corneal thickness, CCT [μm])를 각각 측정하였다.
통계학적 분석은 SPSS for windows (version 24.0, IBM Corp., Armonk, NY, USA)를 이용하였으며, 두 장비 간 일치도는 Bland-Altman analysis 및 급내상관계수(intraclass correlation coefficient)를 이용하여 분석하였다. 95% 일치도 범위(limits of agreement [LOA] mean ± 1.96 standard deviation)를 설정하여 장비 간 호환성 여부를 평가하였으며, 급내상관계수의 경우 0.4 미만일 경우 좋지 않음(poor), 0.4 이상 0.6 미만일 경우 보통(fair), 0.6 이상 0.75 미만일 경우 좋음(good), 0.75 이상일 경우 매우 좋음(excellent)으로 분류하였다. 두 장비의 측정값에 대해 Wilcoxon signed rank test를 시행하여 장비 간 통계적으로 유의한 차이가 있는지 확인하였고 p-value가 0.05 미만인 경우 통계적으로 유의하다고 판단하였다.
결 과
총 43명, 65안을 대상으로 하였으며 이 중 남성은 12명, 여성은 31명이었다. 평균 연령 60.93 ± 16.33세, logarithm of minimal angle of resolution 최대교정시력 0.40 ± 0.47이었으며 현성굴절검사에서 평균 구면렌즈대응치는 -2.67 ± 4.79 D였다(Table 1).
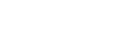
Anterion®으로 측정한 각막 전면의 곡률값은 각각 43.18 ± 2.55 D (anterior flat K, K1), 44.20 ± 2.63 D (anterior steep K, K2), 43.75 ± 2.49 D (anterior mean K), Pentacam HR®으로 측정한 값은 각각 43.31 ± 2.54 D (anterior K1), 44.22 ± 2.57 D (anterior K2), 43.80 ± 2.47 D (anterior mean K)였으며 두 기기 간 평균 차이(mean difference)는 각각 -0.13 ± 0.34, -0.02 ± 0.33, -0.05 ± 0.31이었다(Table 2, 3). Bland-Altman plots 일치도 분석 결과 측정값 간의 95% 일치도 범위는 anterior K1 (-0.81, 0.54), anterior K2 (-0.67, 0.63), anterior mean K (-0.67, 0.56)였으며, 급내상관계수는 각각 0.995, 0.996, 0.996이었다(Table 3, Fig. 1A-C). Anterior K1은 두 기기 간 통계적으로 유의한 차이를 보였으나(p=0.003), anterior K2 및 anterior mean K는 통계적으로 유의한 차이를 보이지 않았다(p=0.789, p=0.217) (Table 2).
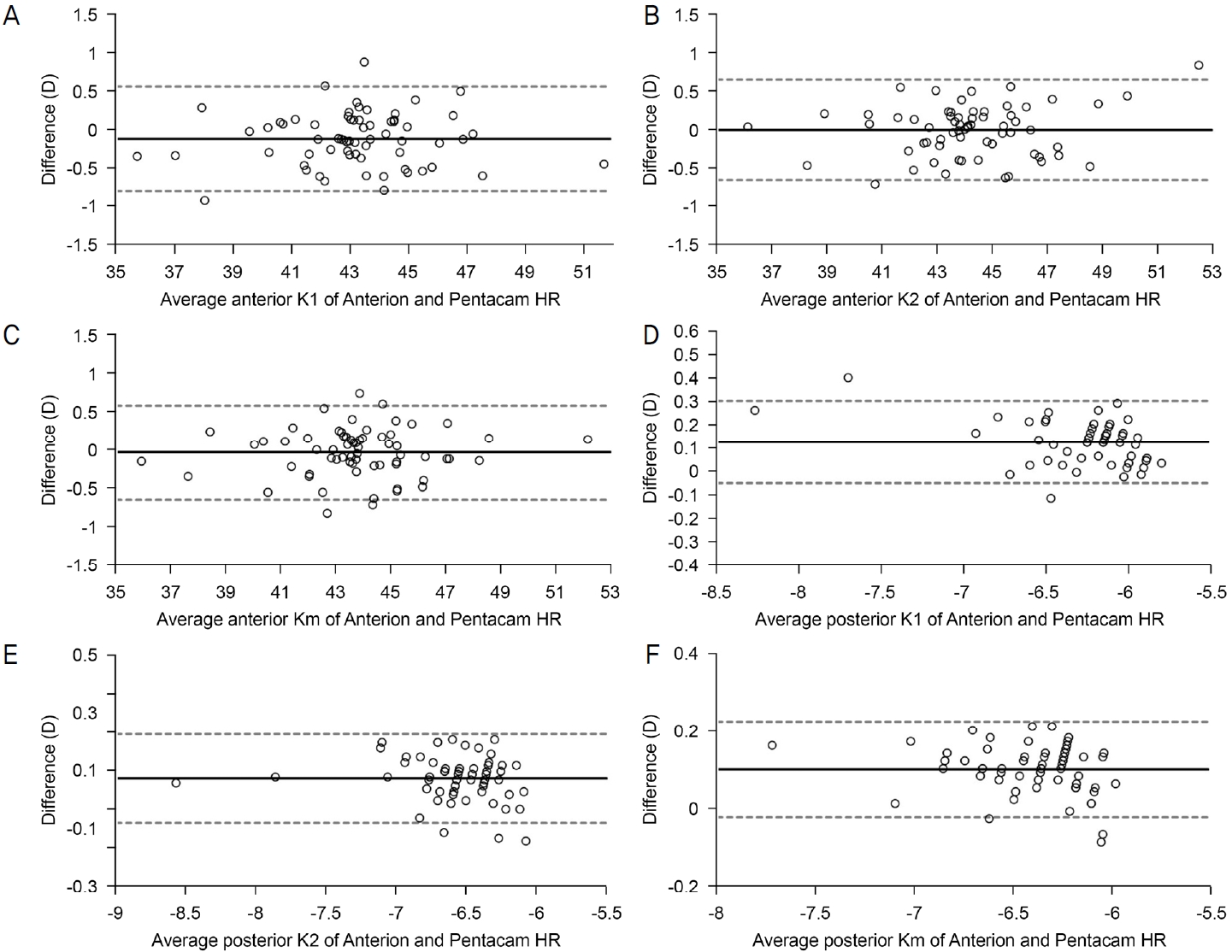
Anterion®과 Pentacam HR®으로 측정한 각막 전면의 J0 (anterior J0)는 각각 -0.08 ± 0.33 D, -0.04 ± 0.35 D, J45 (anterior J45)는 각각 -0.09 ± 0.42 D, -0.03 ± 0.36 D였다(Table 2). 두 기기 간 평균 차이는 각각 -0.03 ± 0.39, -0.06> ± 0.35였으며, 측정값 간 95% 일치도 범위는 anterior J0 (-0.81, 0.74), anterior J45 (-0.75, 0.63), 급내상관계수는 각각 0.905, 0.751이였다(Table 3, Fig. 2A, B). 측정값은 두 기기 간 통계학적으로 유의한 차이를 보이지 않았다(p=0.626, p=0.116) (Table 2).
Anterion®으로 측정한 각막 후면의 곡률값은 각각 -6.21 ± 0.38 D (posterior K1), -6.55 ± 0.39 D (posterior K2), -6.35 ± 0.30 D (posterior mean K), Pentacam HR®으로 측정한 값은 각각 -6.33 ± 0.42 D (posterior K1), -6.62 ± 0.40 D (posterior K2), -6.45 ± 0.32 D (posterior mean K)였으며 두 기기 간 평균 차이는 0.12 ± 0.09, 0.07 ± 0.08, 0.10 ± 0.06이었다(Table 2, 3). 측정값 간 95% 일치도 범위는 posterior K1 (-0.06>, 0.30), posterior K2 (-0.09, 0.22), posterior mean K (-0.03, 0.22)였고, 급내상관계수는 각각 0.987, 0.990, 0.989였다(Table 3, Fig. 1D-F). 측정값은 모두 두 기기 간 통계적으로 유의한 차이를 보였다(p<0.001, p<0.001, p<0.001) (Table 2).
Anterion®과 Pentacam HR®으로 측정한 각막 후면의 J0 (posterior J0)는 각각 -0.03 ± 0.11 D, 0.01 ± 0.15 D, J45 (posterior J45)는 각각 -0.01 ± 0.10 D, 0.01 ± 0.11 D였다 (Table 2). 두 기기 간 평균 차이는 각각 -0.02 ± 0.14, 0.01 ± 0.16이었으며, 측정값 간 95% 일치도 범위는 posterior J0 (-0.30, 0.25), posterior J45 (-0.31, 0.32), 급내상관계수는 각각 0.268, 0.366이었다(Table 3, Fig. 2C, D). 측정값은 두 기기 간 통계학적으로 유의한 차이를 보이지 않았다(p=0.327, p=0.608) (Table 2).
고 찰
최근 백내장수술이 잔여 굴절력을 줄여 최대 나안시력을 얻는 것을 목표로 발전함에 따라 최적의 굴절 결과를 얻기 위한 정확한 전안부 생체계측의 중요성이 대두되고 있다. 특히 도난시 혹은 사난시 환자, 과거 각막굴절교정수술을 받은 환자에서는 각막 후면의 곡률 및 두께를 포함하는 총 각막곡률값을 사용한 인공수정체 도수 계산 공식이 사용되고 있으며, Kim et al16은 백내장수술을 시행한 환자에서 Pentacam HR® 및 Cassini를 사용하여 전안부를 계측하였을 때 두 기계 모두 각막의 전면 난시보다 후면 난시를 포함한 전체 난시가 굴절난시와 일치하여 정확도가 증가하는 결과를 보였다고 보고하였다. 각막 후면을 측정 가능한 장비로는 샤임플러그 카메라 방식의 Pentacam HR®, SIRIUS® 와 파장가변 빛간섭단층촬영계인 IOL Master 700®, Anterion® 등이 있다.
Pentacam HR® (OCULUS)은 샤임플러그 카메라 방식의 세극등 원리를 이용한 기기로 한 대의 카메라가 360° 회전하면서 각막 전, 후면의 elevation map을 얻어 각막 형태를 분석하여 각막곡률을 산출하고 이를 통해 각막 전, 후면의 고위 수차를 산출할 수 있는 각막지형도 검사기이다.12 Anterion®(Heidelberg Engineering Inc.)은 최근 새롭게 도입된 파장가변 빛간섭단층촬영계(swept-source optical coherence tomography) 로 파장가변 빛간섭단층촬영기와 적외선 카메라로 구성되어 있으며, 1,300-nm wave-length swept laser를 이용하여 3차원 상을 만들어낸다. 10 μm 미만의 축방향 해상도(axial resolution)를 가지고 16.5 mm의 폭과 14 ± 0.5 mm 깊이까지 안구 B-scan 영상을 제공하며, 긴 파장의 광원으로 전안부 전체를 분석할 수 있다.13
IOL Master 700® (Carl Zeiss Meditech AG)은 파장가변 빛간섭단층촬영계로 1,050-nm wave-length swept laser를 사용하며 2,000 A-scans/s의 속도로 전체 안구의 tomogram을 획득 가능한 장비로,11 2017년 Shajari et al14은 백내장수술이 예정된 환자 70명, 79안을 대상으로 한 전향적 연구에서 안구 길이, 각막곡률, 전방깊이 측정값에 있어 Pentacam HR AXL, IOL Master 700, IOL Master 500 세 기기 간 통계적으로 유의한 차이가 없음을 발표하였다.
2022년 Pfaeffli et al15은 백내장수술이 예정된 환자 78명, 78안을 대상으로 한 단면 조사연구에서 IOL Master 700®과 Anterion®의 측정값 비교 시 전방깊이 및 수정체 두께 평균값에서 유의한 차이를 보였으나, 두 기기 간 측정값의 일치도는 높음을 보고하였다. 또한, 각각의 기기를 사용한 인공수정체 도수 계산 시 두 기기 간 유의한 차이가 없음을 밝혔다.
국내에서는 2020년 Kim et al16이 Anterion®과 IOL Master 500®의 전안부 계측치를 비교하여 각막곡률 및 안축장에서 높은 일치도를 보고하였고, 2021년 Oh et al17이 Anterion®과 CASIA®, IOL Master 700®의 전안부 계측치를 비교하여 전체 각막곡률을 제외한 각막곡률, 안축장, 수정체 두께, 중심각막두께, 전방깊이에서 높은 일치도를 보고하였다. 저자들이 아는 바에 따르면 국내에서 Anterion®과 Pentacam HR®의 전안부 계측치를 비교한 연구가 없었기에, 본 연구에서는 Anterion®과 Pentacam HR®으로 측정한 여러 각막계측치 간 일치도를 비교하여 새로 개발된 파장가변 빛간섭단층촬영계인 Anterion®의 정확성 및 임상적 유용성을 알아보고자 하였다.
본 연구에서 Anterion®과 Pentacam HR®으로 측정한 전안부 계측치 간 일치도를 Bland-Altman plot으로 나타냈을 때 산점도는 대부분 오차 범위(95% 일치도 한계) 내에 존재하였으나 다소 산발적인 분포를 보였다. 급내상관계수의 경우 각막 후면의 J0 및 J45를 제외한 전안부 계측치에서 0.75 이상으로 “매우 좋음”에 해당하였으며, 그중 각막 전면의 J45 외에는 모두 0.9 이상으로 확인되었다. Wilcoxon signed rank test에서 각막 전면 가파른 축의 곡률과 평균 곡률, 각막 전면 및 후면의 난시값은 두 기기 간 통계적으로 유의한 차이를 보이지 않았다. 반면 각막 전면 편평한 축의 곡률, 각막 후면 곡률, 전방깊이 및 중심각막두께에서는 두 기기 간 통계적으로 유의한 차이를 보였다.
Anterion과 Pentacam의 측정값을 비교 분석한 Tañá-Rivero et al,18 Pérez-Bartolomé et al19의 연구 결과와 비교하였을 때, 본 연구에서 두 기기 간 각막곡률 측정값의 평균 차이 및 95% 일치도 한계는 이전 연구와 비슷하게 확인되며 급내상관계수 또한 모두 0.9 이상으로 확인되었으나, 각막 전면의 편평한 축 및 평균 곡률 외에서는 기기 간 통계적으로 유의한 차이를 보였다(p<0.005). Pentacam HR®은 회전하는 카메라를 이용하여 각막 전면 및 후면에서 얻은 elevation map으로 3차원 구조를 만들어내며 이를 통해 각막 곡률을 산출하는 반면, Anterion®에서는 총 65개의 방사형 이미지를 측정하여 3 mm 중심각막곡률값을 산출하므로 이러한 방식의 차이가 두 기기 간 각막곡률 측정값의 차이를 유발하였다고 생각해볼 수 있겠다.
각막 전면 및 후면 난시의 경우 기기 간 통계적으로 유의한 차이는 확인되지 않았다. 각막 전면 난시의 기기 간 측정값 비교 시 급내상관계수는 0.75 이상이었으나 이전 연구18와 비교 시 평균 차이가 더 크게 나타났으며 95% 일치도 한계 또한 큰 범위로 나타났다. 각막 후면 난시의 기기 간 측정값 비교 시 평균 차이 및 95% 일치도 한계는 크지 않았으나 급내상관계수 0.4 미만으로 “좋지 않음”에 해당하였다. 동일한 샤임플러그 카메라 방식을 사용하는 SIRIUS®와 Pentacam HR® 간 전안부 계측치를 비교 분석한 이전 연구에서 기기 간 이동하며 측정안 정렬이 달라지거나 동공 중심에서 이탈되는 정도에 따라 측정값이 달라질 수 있다고 하였다.20 본 연구에서도 서로 다른 두 기기 간 이동을 하며 측정하였고 반복 측정 없이 단 1회의 측정만 시행하였기에, 이동 과정에서 측정안의 정렬 변화가 난시 측정값의 차이를 유발하였을 수 있다. 2017년 Sel et al21은 Pentacam HR AXL과 IOL Master 700의 전안부 계측값을 비교한 연구에서 J0, J45의 기기 간 측정값의 95% 일치도 한계를 각각 -0.18 to 0.23, -0.18 to 0.21로 보고하였으며, 95% 일치도 한계가 좁기에 각 기기의 측정값을 상호 교환적으로 사용할 수 있다고 주장하였다. Pentacam HR과 IOL Master 700의 측정값을 비교한 Özyol and Özyol22의 연구에서 J0, J45의 95% 일치도 한계는 각각 (-0.10, 0.24), (-0.31, 0.27)로 마찬가지로 95% 일치도 한계가 좁아 기기 간 측정값을 상호 교환적으로 사용할 수 있다고 주장하였다. 본 연구에서 95% 일치도 한계는 anterior J0 (-0.81, 0.74), anterior J45 (-0.75, 0.63), posterior J0 (-0.30, 0.25), posterior J45 (-0.31, 0.32)로 두 기기 간 측정값을 상호 교환적으로 사용하기는 어렵다.
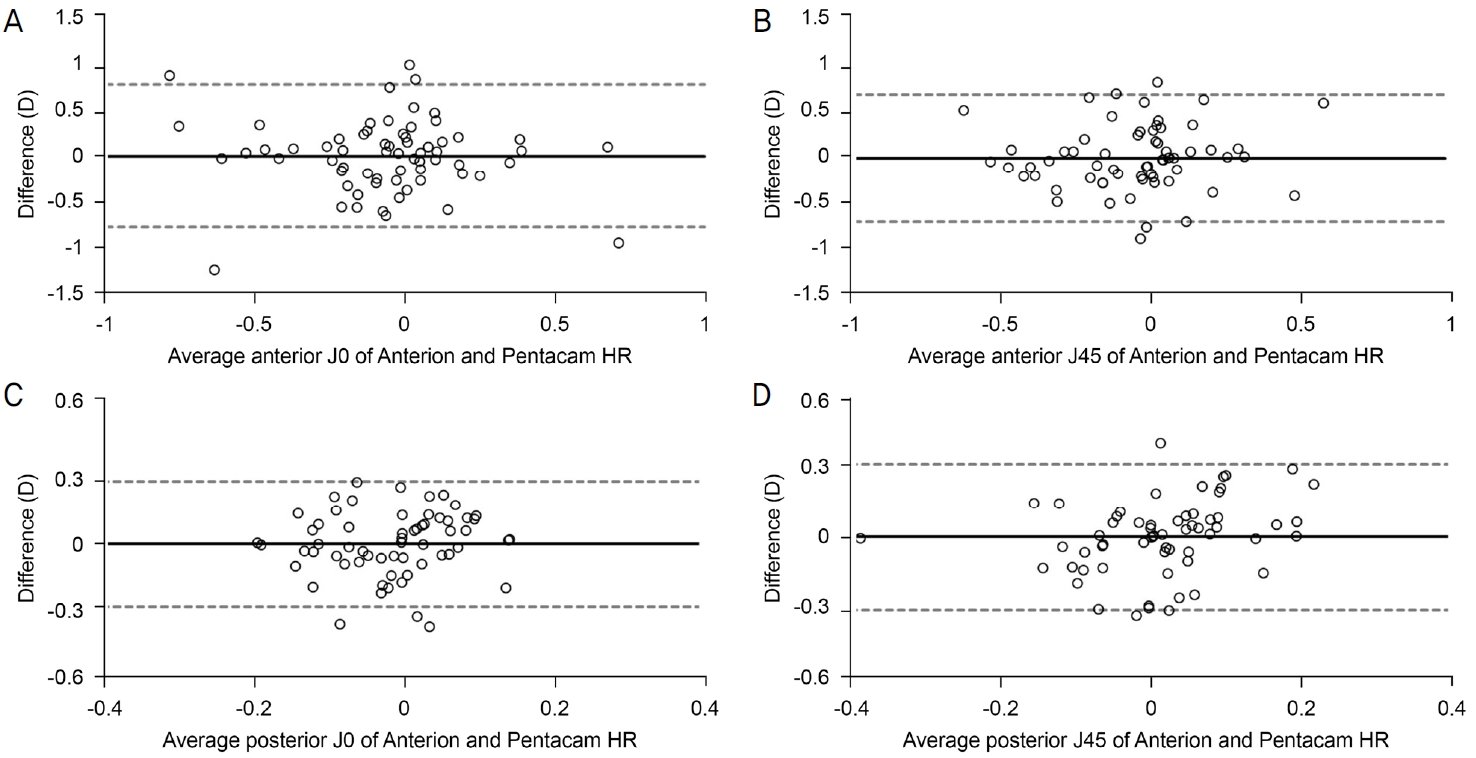
전방깊이는 각막 중앙의 각막내피 정점에서 수정체 전낭 표면의 정점까지의 거리로 샤임플러그 방식의 기기인 Pentacam HR®은 회전하는 카메라에 의해 얻어진 상을 이용하여 전방의 모양을 재구성하여 전방깊이를 측정하며, Anterion®은 시축을 따라 각막 후면 중심에서부터 수정체 전면 중심까지의 거리인 방수 깊이를 측정한 후 중심각막두께를 합하여 산출한다.23 두 기기 간 측정값의 평균 차이 및 95% 일치도 한계는 이전 연구18와 비슷하였고 급내상관계수 0.9 이상으로 확인되었다.
중심각막두께는 각막 중앙의 각막상피에서 각막내피까지의 거리로 샤임플러그 방식의 기기인 Pentacam HR®은 회전하는 카메라에 의해 얻어진 각막 전, 후면의 융기를 측정하는 지점을 기반으로 공기-눈물막 경계 면에서 각막 후면 표면 사이의 각막두께를 측정하며, Anterion®은 빛간섭단층촬영계로 각막의 전면과 후면을 식별하여 각막 전면의 정점으로부터 각막 후면 표면 사이의 수직 거리를 측정한다.24 Lu et al25은 빛간섭단층촬영계에 의해 식별된 각막 전면의 경계면은 실제 각막 전면 표면보다 약간 후방에 위치될 수 있으며 각막두께의 과소 측정으로 이어질 수 있다고 하였다. 본 연구에서 중심각막두께의 기기 간 평균 차이는 -3.51 ± 7.42로 Anterion®에서 Pentacam HR®보다 작게 측정되었고 이러한 차이는 측정 방식의 차이에서 유발되었을 것으로 생각할 수 있다. 두 기기 간 평균 차이 및 95% 일치도 한계는 이전 연구18,19와 비슷하게 나타났으며 급내상관 계수 0.9 이상으로 확인되었다.
본 연구의 제한점으로는 첫째로 별다른 제외 기준 없이 Anterion®과 Pentacam HR®을 모두 시행한 환자들을 대상으로 하여 백내장이 아주 심하거나 건성안 등 눈물막에 영향을 줄 수 있는 질환이 있는 환자들도 모두 포함되어 부정확한 계측값이 도출되었을 가능성이 있다. 둘째, 서로 다른 두 기관에서 다른 검사자에 의해 측정된 데이터를 분석하였으나 각 기기들의 반복성 및 재현성에 대한 검증을 시행하지 않았다는 것이다. 기존 연구들에서 Anterion®과 Pentacam HR® 모두 정상안에서 높은 반복성 및 재현성이 증명되었으나26,27 본 연구는 심한 백내장, 안구건조, 원추각막 등 질환이 있는 경우도 포함하였기에 여전히 제한점이 있겠다. 셋째, 본원에서 보유 중인 Pentacam HR® 장비로는 안축장(axial length)과 수정체두께(lens thickness)를 측정할 수 없어 비교가 불가능하였고 넷째, 전방깊이의 경우 대상자 수가 36안으로 적었다. 그러나 Tañá-Rivero et al18이 보고한 평균 차이 및 표준편차(Table 4)를 사용하여 최소 표본 수 계산 시 31안일 경우 80% 이상의 통계 검증력이 확보되며, 국내에서는 처음으로 Anterion®과 Pentacam HR®의 측정값을 비교 분석한 연구라는 점에서 의의가 있다.
결론적으로 본 연구에서 Anterion®과 Pentacam HR®의 측정값 비교 시 차이의 절대값은 크지 않았고 선행 연구들과 유사한 평균 차이 및 95% 일치도 한계를 보였다(Table 4). 또한, 각막 전면 J45와 각막 후면 J0 및 J45를 제외한 계측치에서 급내상관계수는 0.9 이상이었으나 Bland-Altman plot에서 다소 산발적인 분포를 보였다. 두 기기 간 측정값을 상호 교환적으로 사용하기 위해서는 95% 일치도 범위를 고려해야 하며, 측정값 간 통계적으로 유의한 차이를 보이더라도 그 차이가 인공수정체 도수 계산에 미치는 영향이 무시할 수 있을 정도인 경우 상호 교환 가능 여부에 대해서는 반드시 임상적 판단이 동반되어야 한다. 이러한 결과를 뒷받침하고 한계점을 보완하기 위해서는 정상 범위를 벗어나는 측정값을 보인 환자군 및 일치도가 낮은 환자군에 대한 개별화된 연구와 질환별 연구 그리고 더 많은 환자들을 대상으로 한, 잘 설계된 전향 연구가 필요하겠다.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






