양안성 미만성 포도막 멜라닌세포 증식증으로 나타난 샘암종
An Adenocarcinoma Associated with Bilateral, Diffuse, Uveal Melanocytic Proliferation
Article information
Abstract
목적
양안 미만성 포도막 멜라닌세포 증식증으로 나타난 위 샘암종 증례를 보고하고자 한다.
증례요약
78세 남자가 3개월 전 발생한 양안 시력저하 주소로 내원하였다. 당뇨 외 특이 병력은 없으며, 4년 전 양안 백내장수술을 받았다. 교정시력은 우안 안전수지, 좌안 20/160로 측정되었고, 안압 및 전안부는 정상이었다. 양안 안저에서 여러 개의 둥근 모양의 반점이 후극부에 관찰되었고, 망막하 망막색소상피 과색소 및 탈색소 병변이 동반된 삼출망막박리가 관찰되었다. 빛간섭단층촬영에서 색소성 병변은 시세포와 망막색소상피 사이에서 과반사를 보이는 망막하 삼출물로 확인되었고 망막하액과 망막내액이 관찰되었다. 양안 미만성 포도막 멜라닌세포 증식증으로 진단 후 영상학적 전신 평가를 시행하였다. 복부 컴퓨터 전산화단층촬영에서 악성종양으로 의심되는 종괴가 다수 관찰되었다. 상부위장관 내시경 조직검사를 시행 후 샘암종으로 진단되었다.
결론
원발악성종양에 의해 이차적으로 발생한 양안 미만성 포도막 멜라닌세포 증식증은 다발성의 색소성 망막하 삼출물을 동반한 삼출망막박리로 나타나며, 이와 같은 안저 소견을 보이는 환자에서는 전신검사를 통해 악성종양에 대한 평가가 필요하다.
Trans Abstract
Purpose
We report bilateral, diffuse, uveal melanocytic proliferation caused by a stomach adenocarcinoma.
Case summary
A 78-year-old male complained of visual impairment 3 months in duration. He had diabetes and had undergone cataract surgery on both eyes 4 years prior. His best-corrected visual acuity was counting fingers in the right eye and 20/160 in the left eye. Both intraocular pressures were normal. The anterior segments yielded no specific findings. The maculae exhibited multiple, round, patchy, pigmented or depigmented lesions with exudative retinal detachment. Fluorescein angiography revealed multiple hyperfluorescent lesions. Optical coherence tomography revealed that the hyper-reflective exudates lay between the neurosensory retina and the retinal pigment epithelium. We diagnosed bilateral, diffuse, uveal melanocytic proliferation and performed a systemic evaluation. Computed tomography revealed several mass lesions in the lung, stomach, and lymph nodes; these appeared to be malignant. An esophagogastroduodenoscopic biopsy confirmed that the lesions were adenocarcinomas.
Conclusions
A bilateral, diffuse, uveal melanocytic proliferation induced by a primary malignant tumor exhibited multiple, pigmented subretinal exudates associated with exudative macular retinal detachment. In patients with such findings, it is necessary to evaluate the malignant tumor status of remote organs.
원발장기의 악성종양에 의해 이차적으로 발생할 수 있는 부종양증후군(paraneoplastic syndrome)은 다양한 장기에 다양한 소견으로 나타날 수 있다. 부종양증후군은 종양에서 분비되는 호르몬이나 성장인자가 타 장기에 영향을 끼쳐 발생할 수 있으며(예, 쿠싱증후군, 부갑상선 호르몬 관련 과칼슘혈증 등), 또한, 종양항원과 정상 조직과의 면역 관련 교차반응에 의해 발생할 수도 있다(예: Lambert-Eaton myasthenic 증후군, paraneoplastic cerebellar degeneration 등). 정확한 유병률 및 발병률은 알 수 없으나 암 환자의 약 10%에서 발생하는 것으로 추정된다[1]. 하지만, 시각 신경계를 침범하는 경우는 아주 드물어, 암 전문 삼차의료기관을 방문한 암 환자에서 약 0.01%에서 경험하는 것으로 알려져 있다[1]. 안구 관련 대표적인 부종양증후군으로는 암 관련 망막병증(cancer-associated retinopathy, CAR), 흑색종 관련 망막병증(melanoma-associated retinopathy, MAR), 부종양성 노른자모양 망막병증(paraneoplastic vitelliform maculopathy, PVM), 양안성 미만성 포도막 멜라닌세포 증식증(bilateral diffuse uveal melanocytic proliferation, BDUMP) 등이 있다[2]. 그중에서도 양안성 미만성 포도막 멜라닌세포 증식증은 다른 부종양증후군들에 비해 더욱 드문 안과적 부종양증후군이다. 양안의 다발성, 오렌지 색의 색소성 망막하 침윤과 삼출망막박리 등의 특징적인 안저 소견으로 진단할 수 있으며, 이러한 안저 소견이 있는 환자에서는 원발 장기의 악성종양을 반드시 의심해보아야 한다[3-5]. 본 저자들은 안구 내 종양으로 의뢰된 78세 환자에서 양안성 미만성 포도막 멜라닌세포 증식증으로 진단하고 소화기계의 악성샘종을 진단한 증례를 경험하여 보고하고자 한다.
증례보고
78세 남자가 3개월 전부터 발생한 양안 시력저하를 주소로 내원하였다. 당뇨 외에는 특이 병력은 없으며, 4년 전에 양안 백내장수술을 받았었다. 교정시력은 우안 안전수지, 좌안 20/160이고, 안압은 양안 10 mmHg였다. 홍채 및 섬모체 부분을 포함해서 전안부에는 특이 소견이 없었다. 안저검사에서 반점 형태의 과색소 병변을 동반한 삼출망막박리가 양안에서 관찰되었다. 유리체의 염증세포는 없었다(Fig. 1A-D). 광각안저혈관조영에서는 초기부터 양안 다수의 과형광의 누출이 관찰되었다(Fig. 1E, F). 색소성 병변은 빛간섭단층촬영에서 시세포 아래와 망막색소상피 위에 과반사를 보이는 망막하 삼출물로 확인되었으며, 망막색소상피박리와 망막하액, 망막내액이 함께 관찰되었다(Fig. 2). 양안성 미만성 포도막 멜라닌세포 증식증(bilateral diffuse uveal melanocyte proliferation)이 의심되었다. 원발 장기의 악성종양에 의한 부종양증후군(paraneoplastic syndrome)을 감별하기 위해 전혈구수, 간 및 신장기능에 대한 혈액검사와 함께 영상학적 검사를 시행하였다. 혈액검사에서는 특이 소견이 없었으나, 안와 조영증강 자기공명영상촬영에서는 전이성 종양은 없었고, 양안 안구후벽에 과반사의 편평한 병소가 관찰되었다(Fig. 3A). 흉부 및 복부 컴퓨터 전산화단층촬영에서는 폐, 위와 다수의 림프절에 악성종양으로 의심되는 병소들이 확인되었다(Fig. 3B). 소화기내과에서 시행한 상부위장 내시경검사에서 식도에 1 cm가량의 검은색 색소침착 병변 관찰되었고, 위 체부 소만에 7 cm가량의 불규칙한 변연을 가진 깊은 궤양성 병소가 관찰되었다(Fig. 4). 식도의 색소성 병변과 위 체부 소만의 궤양성 병변에서 조직검사를 시행하였고, 샘암종(adenocarcinoma)으로 진단되었다. 타 장기로의 원격 전이가 있었으므로 미국 암 연합위원회(American Joint Committee on Cancer)의 진단 기준에 따라 위암 4기에 해당하였다. 상기의 증례는 샘암종에 의한 부종양증후군으로 발생한 양안성 미만성 포도막 멜라닌세포 증식증으로 확진되었다. 환자는 향후 안과적 치료 및 전신 항암치료를 원하지 않아 대증요법을 포함한 완화 치료로 경과 관찰하기로 하였다.
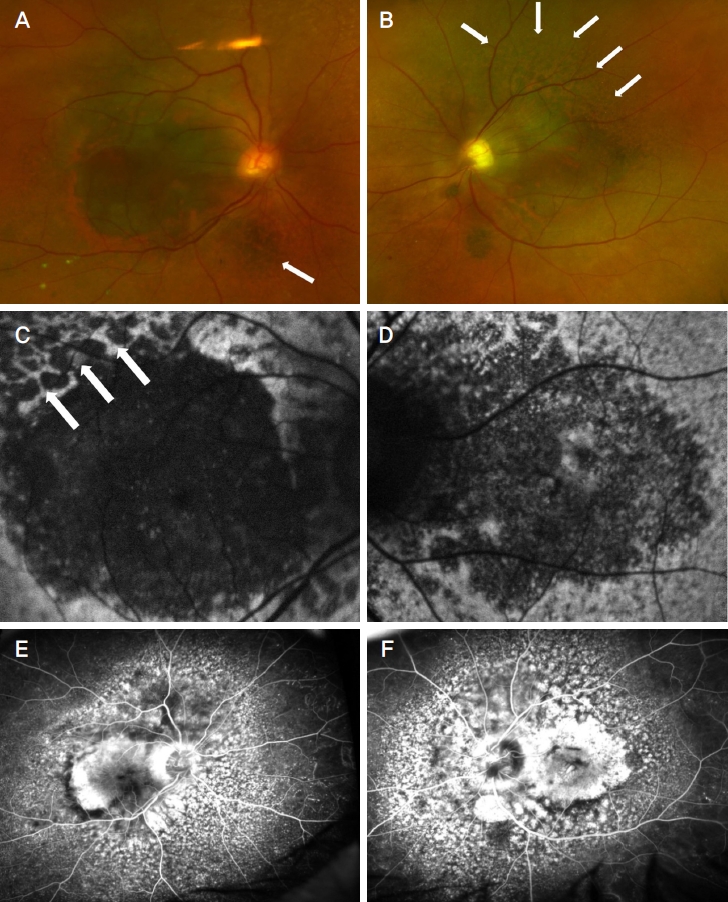
The patient’s fundus photographs. (A) Photograph showed multiple round-shaped pigmentary lesions and serous retinal detachment on macula. Unique giraffe pattern (white arrows) in right and (B) left eye. (C) Fundus autofluorescence photograph presented autofluorescence pattern with giraffe pattern (white arrows) in right eye and (D) left eye. (E) Wide-field fluorescein angiography presented multiple hyperfluorescent leakages in right and (F) left eye.
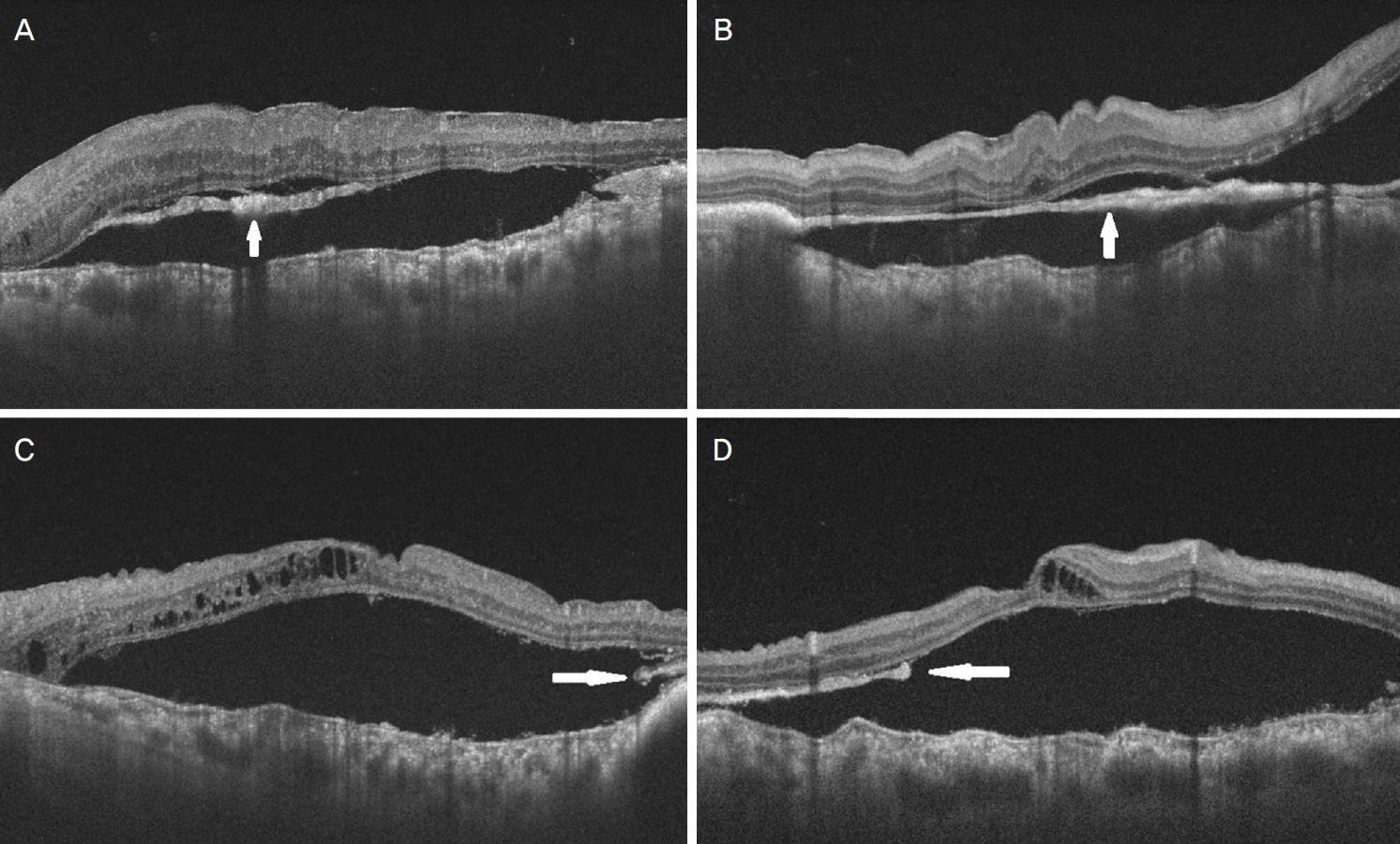
The optical coherence tomography images of macula. The subretinal hyper-reflective exudates (white arrows), serous retinal detachment, and undulated thick choroid were observed in both eyes. (A) The subretinal fluid and hyper-reflective exudates (white arrows) were in the horizontal and (B) vertical scan images of the right eye. (C) The subretinal and intraretinal fluids with subretinal exudates in the horizontal and (D) vertical scan images of left eye.

The orbital magnetic resonance and abdominal computer tomography images. (A) Flat T2 high signal intense at the posterior walls of the bilateral eyeballs (white arrows) were observed in both eyes. (B) Multiple metastatic lymph nodes (white arrows) were at the paraaortic area.

Esophagogastroduodenoscopy image showed that lesser curvature of stomach with 7 cm of uneven margin and central ulcerofungating lesions. The adenocarcinoma was confirmed by the biopsy specimen.
고 찰
안과적으로 발생하는 부종양증후군에는 암 관련 망막병증, 흑색종 관련 망막병증, 부종양성 노른자모양 망막병증, 양안성 미만성 포도막 멜라닌세포 증식증 등이 있는데, Barr et al [6]에 의해 처음 보고된 양안성 미만성 포도막 멜라닌세포 증식증은 그중에서도 매우 드문 질환이다. 본 증례와 같이 소화기계의 악성종양으로 인해 발생할 수도 있으며 직장, 대장, 췌장, 신장, 폐, 담낭 등 다양한 장기의 원발악성종양이 원인이 될 수 있다[7]. 양안성 미만성 포도막 멜라닌세포 증식증과 가장 관련이 있는 원발종양은 여성에서는 난소암과 같은 부인과암이, 남성에서는 췌장암과 폐암이라고 보고된 적이 있다[8].
양안성 미만성 포도막 멜라닌세포 증식증은 망막 광수용체의 손상과 삼출망막박리, 빠르게 진행하는 백내장으로 인해 시력저하가 발생한다. 위축된 망막색소상피와 그에 인접한 과증식된 망막색소상피로 인해 나타나는 독특한 기린 형태(giraffe pattern)의 안저는 이 질환을 진단하는 데 특징적인 소견이다. Gass et al [3]는 양안성 미만성 포도막 멜라닌세포 증식증의 5가지의 특징적인 안저와 검사 소견을 다음과 같이 정리하였다: 1) 다발성, 둥근 오랜지-적색의 망막하 반점, 2) 형광안저혈관조영술에서 초기부터 나타나는 과형광 소견, 3) 전반적으로 두꺼워진 맥락막과 함께 국소적으로 융기된 과색소 및 탈색소된 포도막 멜라닌세포 종양(uveal melanocytic tumor), 4) 삼출망막박리, 5) 빠른 진행성 백내장. 본 증례는 4년 전 백내장수술을 이미 받아 그 진행 양상은 확인할 수 없었으나, 양안의 안저에 다발성 색소성 반점, 삼출망막박리, 형광안저혈관조영에서 누출, 두꺼워진 맥락막과 맥락막 융기가 모두 관찰되어 양안성 미만성 포도막 멜라닌세포 증식증으로 진단할 수 있었다. 원발종양은 상부위장관에서 조직검사를 통해 샘암종(adenocarcinoma)으로 진단되었다. 양안성 미만성 포도막 멜라닌세포 증식증은 위에서 언급한 5가지 특징적인 안저 소견 중에서 과색소 및 탈색소 병변은 비교적 다양하게 보고되었는데, 상대적으로 멜라닌세포의 색소성 증식이 심한 경우에서는 과색소 병변이 뚜렷하며, 망막색소상피의 위축이 심한 경우에는 탈색소성의 위축성 병변이 함께 관찰될 수 있다[9]. 특히 색소성 병변이 더욱 뚜렷한 부종양성 멜라닌세포 증식은 super nevus라고 언급되기도 하는데, 본 증례처럼 과색소성의 병소가 상대적으로 뚜렷한 양안성 미만성 포도막 멜라닌세포 증식증이 발생한 경우로는 신장의 샘암종 증례와 자궁내막의 투명세포암종 증례가 보고된 바 있다[9,10]. 국내에서는 Kim and Yu [11]은 47세의 간세포암 환자에서 양안성 미만성 포도막 멜라닌세포 증식증에 대한 증례에 대해 보고한 바 있는데, 처음에는 안저에서 장액망막박리가 동반된 옅은 회갈색의 병소가 시간이 지나면서 병변의 크기 및 수가 증가하면서 서로 융합하여 둥근 타원형의 병소들이 저명하게 관찰할 수 있었다. 삼출망막박리는 일반적으로 망막하액으로 나타나는 경우가 흔하지만, 본 증례처럼 망막하액과 망막내액이 함께 관찰되는 경우도 보고된 바 있었다[12]. 양안성 미만성 포도막 멜라닌세포 증식증에서 다양한 안저 소견이 나타나는 것은 원발암의 종류, 질병의 유병 기간, 멜라닌세포의 면역 반응 정도에서 차이에서 나타날 수 있다고 생각된다. 이에 대해서는 추가적인 연구가 필요하다.
아직까지 양안성 미만성 포도막 멜라닌세포 증식증의 발생 기전은 명확히 밝혀지지 않았으나, 원발종양세포에서 생성되는 멜라닌세포 성장인자(melanocytic growth factor)가 혈류를 통해 전신을 순환하면서 눈에는 맥락막의 비대와 멜라닌세포의 과증식에 영향을 주는 것으로 생각된다[9]. 양안성 미만성 포도막 멜라닌세포 증식증 환자에서 발생하는 피부와 점막의 과색소 병변들이 이러한 가설을 뒷받침한다[13]. 삼출망막박리는 혈관-망막 장벽과 망막색소상피의 손상으로 발생하는 것으로 생각된다. 한편, 최근에는 순환 항망막 자가항원(circulating anti-retinal autoantibody)의 존재도 관련된 것으로 알려졌다. 환자의 혈청으로 멜라닌세포를 증식시키고 손상을 유발할 수 있으며 다른 세포에는 영향 없이 멜라닌세포에만 영향을 주었다고 보고되었다[14].
양안성 미만성 포도막 멜라닌세포 증식증의 치료는 원발악성종양에 대한 치료와 함께 눈에 대한 치료를 추가적으로 시행해 볼 수 있으나 시력예후가 아주 불량한 것으로 알려져 있다. 국소 방사선치료, 망막하액배액술, 스테로이드 등이 치료에 시도되었으나 대부분 일시적인 호전을 보인 뒤 실명에 이르는 것으로 보고되었다[4,6]. 환자들의 생존 예후도 대체로 불량한데, 상당히 진행된 원발병소의 악성종양이 발견되거나 타 장기로의 전이가 있는 경우가 많다. 생존 기간의 중간값은 약 15.6개월로 보고된 바가 있으나[9], 원발종양의 상태에 따라 그보다 양호한 경우도 보고된 적이 있다[11].
이밖에 비교적 흔하게 발생하는, 감별해야 하는 안과적 부종양증후군에는 암 관련 망막병증이 있다. 암 관련 망막병증은 원발종양과 관련된 자가항체 recoverin에 의한 면역 반응으로 발생하는 것으로 알려져 있다. 이 항체는 망막의 막대세포와 원뿔세포에 영향을 미치며, 환자는 통증 없는 시력저하, 광시증, 눈부심, 중심 시야의 심한 감소, 야맹증 등의 증상이 발생할 수 있다. 암 관련 망막병증의 안저에서는 망막세동맥의 약화, 시세포층과 망막색소상피층의 위축이 나타난다. 경한 유리체염이나 망막혈관염이 동반될 수도 있다[15]. 한편 항 양극세포 항체(anti-bipolar cell antibody)와 관련된 흑색종 관련 망막병증도 안과적 부종양증후군으로 발생할 수 있다. 암 관련 망막병증과 유사한 안저 소견을 보이며 상대적으로 시력이 양호한 경우가 많다[2]. 이 밖에 망막색소상피와 양극세포에 대한 자가항체와 관련이 있는 부종양성 노른자모양 망막병증도 발생할 수 있는데, 베스트병과 안저 소견이 유사하므로 감별진단이 필요하다. 부종양성 노른자모양 망막병증의 많은 증례가 맥락막 혹은 피부 흑색종 환자에서 발생한 것으로 알려져 있다[2].
본 증례에서는 멜라닌세포 성장인자, 항망막 자가항원검사, 피부병변에 대한 조직검사 등의 추가적인 검사를 환자가 거절하여 시행되지 못하였으나 특징적인 안저 소견으로 양안성 미만성 포도막 멜라닌세포 증식증을 진단할 수 있었으며, 전신검사를 통해 상부위장관의 샘암종을 확인할 수 있었다. 본 증례와 같이 안과적으로 발생할 수 있는 부종양증후군은 원발악성종양과 관련이 있으며, 질병에 대한 정확한 이해와 진단이 필요하다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
정우현 / Woohyun Chung
부산대학교 의과대학 안과학교실
Department of Ophthalmology, Pusan National University College of Medicine
