삼출성 황반변성에서 이중 망막색소상피파열 및 출혈성 망막박리 후 발생한 급성폐쇄각발작
Angle-closure Attack after Retinal Pigment Epithelium Double-tear and Hemorrhagic Retinal Detachment in Exudative Macular Degeneration
Article information
Abstract
목적
거대망막색소상피박리가 동반된 삼출성 황반변성에서 유리체강내 주사 후 이중 망막색소상피파열이 발생하였고 출혈성 망막박리와 급성폐쇄각발작을 치료하였기에 이를 보고하고자 한다.
증례요약
66세 여자가 1달 전부터 시작된 좌안의 시력저하를 주소로 내원하였다. 빛간섭단층촬영과 인도시아닌그린혈관조영술에서 거대망막색소상피박리를 동반한 삼출성 황반변성으로 진단하고 유리체강내 애플리버셉트주입술을 1차 시행하였다. 주사 2주 후 망막색소상피파열이 발생, 이후 2차 주사 4주 후 망막색소상피파열의 범위가 황반부를 포함하여 확대되었다. 3차 주입술 3개월 후 대량의 황반하출혈이 발생하여 4차 주사 시행, 3일 후 안압 60 mmHg 상승과 전방각 폐쇄, 수정체 후면에 접촉되는 출혈성 장액망막박리가 발생하였다. 공막절개술을 이용한 망막하출혈과 망막하액의 배액을 시행하였고, 이후 안압하강과 망막박리의 감소 소견이 보여 경과 관찰 중이다.
결론
삼출성 황반변성에서 유리체강내 주사 후 이중 망막색소상피파열로 진행되는 경우는 매우 드물다. 이중 망막색소상피파열에서 출혈성 망막박리로 발생한 급성폐쇄각발작으로 안압상승을 경험하고 이를 치료하였기에 보고하고자 한다.
Trans Abstract
Purpose
To report a case of acute angle-closure attack resulting from hemorrhagic retinal detachment after a double retinal pigment epithelium (RPE) tear in exudative age-related macular degeneration (AMD) with large pigment epithelial detachment (PED).
Case summary
A 66-year-old female visited with a complaint of poor vision in left eye, which began 1 month prior. She was diagnosed with exudative AMD with a large PED using optical coherence tomography and indocyanine green angiography. Intravitreal aflibercept injection was performed. The RPE tear occurred at 2 weeks after the intravitreal anti-vascular endothelial growth factor injection for AMD, after which the range of the RPE tear expanded and included the macular area at 4 weeks after the second injection. At 3 months after the third injection, massive submacular hemorrhage occurred; aflibercept injection was repeated. At 3 days after the fourth injection, the patient’s intraocular pressure (IOP) was 60 mmHg, and massive hemorrhagic serous retinal detachment and anterior movement of the lens with total angle closure were observed. Therefore, we performed a sclerotomy; a large amount of dark blood and subretinal fluid was drained. The IOP decreased, and the retinal detachment improved somewhat. The patient was kept under observation for careful monitoring of her condition.
Conclusions
It is very rare to experience a double RPE rupture after intravitreal anti-vascular endothelial growth factor injection in AMD. We report on our experience and treatment of acute angle-closure attack. The IOP increased due to hemorrhagic retinal detachment after a double RPE tear over the treatment course.
연령관련황반변성은 사회가 고령화됨에 따라 유병률이 증가하고 있으며, 삼출성 연령관련황반변성의 치료로써 유리체강내 항혈관내피성장인자(anti-vascular endothelial growth factor) 주입술이 늘어나고 있다. 하지만 유리체강내 항혈관 내피성장인자 주입술은 안내염, 열공망막박리, 안압상승의 합병증이 발생할 수 있으며 망막색소상피파열, 거대맥락막박리 및 출혈, 거대망막하출혈 등이 발생하여 심각한 시력손실을 유발할 수 있다[1-3].
망막색소상피파열은 1981년 Hoskin et al [4]에 의해 연령관련황반변성에 동반된 망막색소상피박리 환자에서 발생한 합병증으로 처음 보고되었다. 망막색소상피파열은 맥락막신생혈관, 망막혈관종성증식, 결절맥락막혈관병증에서 자연 경과로 발생하거나, 신생혈관 연령관련황반변성의 광역학치료, 레이저광응고술과 관련하여 발생하기도 한다[5,6].
망막색소상피박리, 망막하액을 동반한 삼출성 연령관련황반변성 환자에서 유리체강내 항혈관내피성장인자 주입술 치료 후 망막색소상피파열이 연속하여 두 번 발생하는 이중 망막색소상피파열은 흔하지 않으며 국내에 보고된 바가 없다. 저자들은 삼출성 황반변성 환자에서 유리체강내 항혈관내피성장인자 주입술 후 이중 망막색소상피파열이 발생하고 이로 인한, 대량의 이차성 출혈망막박리로 급성폐쇄각발작이 유발되어 안압상승이 발생된 환자를 경험하였기에 관련 문헌고찰과 함께 보고하는 바이다.
증례보고
66세 여자가 1달 전부터 시작된 좌안의 시력저하를 주소로 내원하였다. 기저질환으로 고혈압으로 치료 중이었으며, 예방적으로 아스피린을 복용하고 있었다. 본원 내원시 최대교정시력은 우안 20/20, 좌안 20/25이었고, 골드만압평안압계로 측정한 안압은 우안 20 mmHg, 좌안 22 mmHg였다. 안저검사에서 양안 다발성 드루젠 소견을 보였으며, 빛간섭단층촬영에서 망막하액, 좌안의 큰 돔 형태의 망막색 소상피박리가 관찰되었고, 최대직경 5,645 μm, 최대높이 1,045 μm였다(Fig. 1). 형광안저촬영술에서 좌안의 망막하액으로 인한 과형광이 관찰되었고, 인도시아닌그린혈관조영술에서 좌안의 형광차단으로 인한 저형광과 경계 부위에 맥락막신생혈관이 관찰되었다(Fig. 1). 망막색소상피박리가 동반된 삼출성 황반변성으로 진단하고 좌안 유리체강내 애플리버셉트주입술을 시행하였으며, 첫 주사 전 좌안 안압은 20 mmHg였다. 첫 주사 2주 후 망막색소상피파열이 관찰되었으며, 좌안 최대교정시력 20/25, 안압 22 mmHg였고, 주사 4주 후 2차 유리체강내 애플리버셉트주입술을 시행하였다. 2차 주사 4주 후 첫 번째로 발생한 망막색소상피파열에 연결되어 중심와를 포함한 더 넓은 범위의 추가적인 망막색소상피파열이 발생하였고, 좌안 최대교정시력 20/800, 안압 20 mmHg였다(Fig. 2). 2차 주사 4개월 후 황반하출혈 증가 소견이 보여 아스피린을 중단하였으며, 3차 유리체강내 애플리버셉트주입술을 시행하였고 이후 황반하출혈은 감소되었다. 3차 주사 3개월이 되는 시기에 좌안의 시력저하와 함께 대량의 황반하출혈이 발생하여 4차 유리체강내 애플리버셉트주입술을 시행하였다. 4차 주사 3일 후 좌안의 통증으로 내원하여 측정한 최대교정시력은 광각인지, 안압은 60 mmHg로 상승하였으며, 세극등검사에서 각막부종, 홍채 및 수정체 전방이동, 전방각 폐쇄 소견이 보였고, 안저검사에서 수정체 후낭에 접촉되어 있는 심한 출혈성 장액망막박리가 관찰되었다(Fig. 3). 공막절개술을 통한 맥락막 천자술을 시행하여 출혈과 망막하액의 외배액술을 시행하였다. 국소마취하에, 눈 주위 피부에 10% betadine 용액으로 소독한 후 눈벌리개로 눈을 벌려 결막에 5% betadine 용액과 balanced salt solution 용액으로 세척하였다. 결막절개술을 4시에서 8시 방향까지 시행하고, 각막윤부에서 4시와 7시 방향, 8 mm 떨어진 부위에 공막절개를 시행하였다. 얕아진 전방윤부에 부절개를 시행한 후 3 mL 주사기를 통하여 balanced salt solution 용액으로 전방을 세워 섬모체 뒤쪽으로 방수가 흐르도록 하여 망막에 가해지는 압력으로 배액을 유도하였다. 공막절개부에 압력을 가하며 공막절개부를 통하여 검붉은 출혈이 배액되었다. 망막박리의 완화와 전방이 깊게 유지되는 것을 확인하고 공막절개 부위를 6-0 vicryl로 봉합하고 결막봉합 후 수술을 마무리하였다(Fig. 4A). 수술 1일째 안압 11 mmHg로 감소하였으며 이후 망막박리의 감소 소견이 관찰되었다(Fig. 4B). 그러나 수술 2주 후 황반하출혈이 유리체 내로 퍼지는 소견이 보여 유리체절제술을 고려하였으나 환자 수술을 원하지 않아 경과 관찰 중이며 안압의 재상승이나 망막박리의 증가 소견은 보이지 않았다(Fig. 4C).
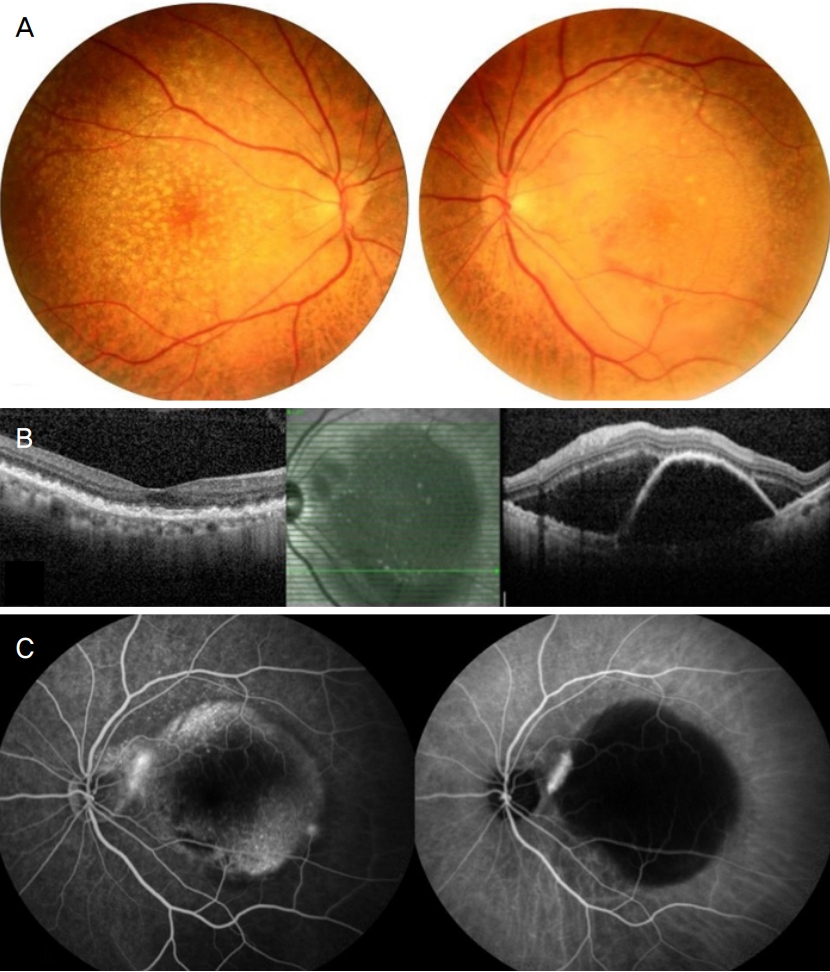
(A) Fundus photographs showing multiple drusens in both eyes and large pigment epithelial detachment (PED) in the left eye at the patient’s first visit. (B) Spectral domain optical coherence tomography showing subretinal fluid and large PED in the left eye at the first visit. (C) Fluorescein angiography and indocyanine green angiography showing hyperfluorescent neovascularization located in the margin of large PED at the baseline evaluation.
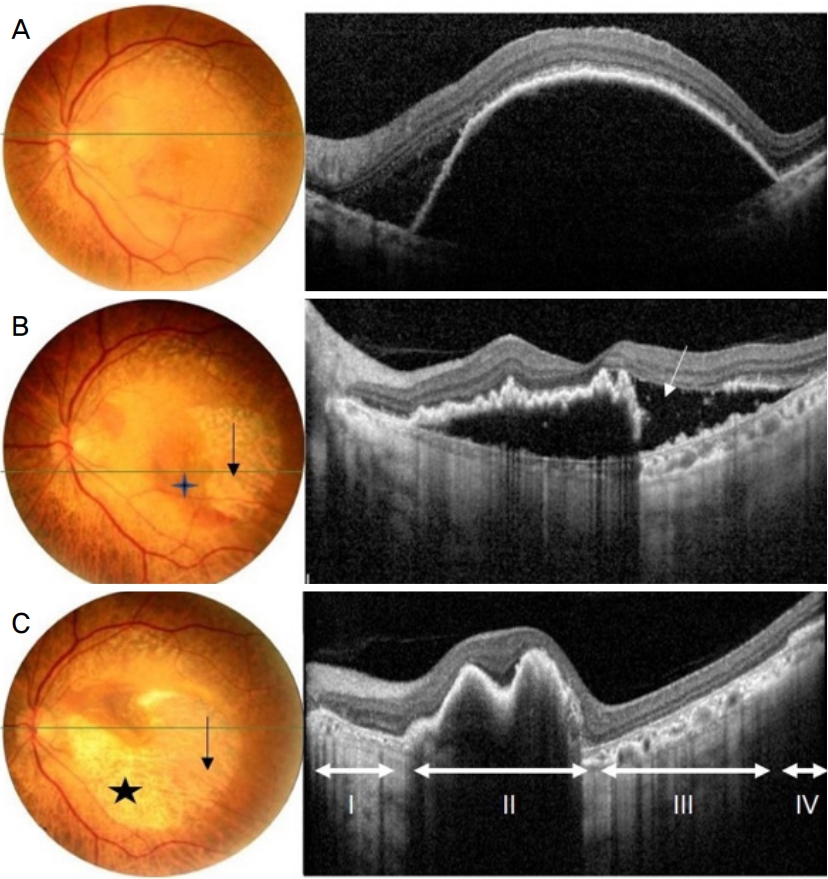
Fundus photograph and Spectral domain optical coherence tomography (SD-OCT) in a 66-year-old female before and after intravitreal injection of anti-vascular endothelial growth factor. (A) The first visit. (B) Two weeks follow-up after the first intravitreal aflibercept injection. In the funduscopic image, the retinal pigment epithelium (RPE) tear appears as an area of depigmented retina (black arrow) where the choroidal vessels are visualized, associated with a hyperpigmented line that corresponds to the rolled RPE (diamond). SD-OCT showed an area devoid of RPE reflectivity with an adjoining area of high reflectivity corresponding to the scrolled margin of the RPE tear (white arrow). (C) Four weeks follow-up after the secondary intravitreal aflibercept injection. In the funduscopic image, the additional RPE tear (black star) appears as an area of depigmented retina connecting with fist RPE tear (black arrow). SD-OCT showed missing RPE band in the additional RPE tear (=double RPE tear) area representing the first part, scrolled RPE in the second part, missiong RPE band in the first RPE tear area representing the third part, normal architecture of the outer retinal bands in the fourth part.

(A) Fundus photograph showing extensive subretinal hemorrhage 3 months after the third intravitreal aflibercept injection. (B) Fundus photograph showing massive hemorrhagic serous retinal detachment 3 days after the fourth intravitreal aflibercept injection. (C) Slit lamp photograph of the anterior segment showing the detatched retina and retinal vessels, as well as corneal diffuse edema. (D) B-scan ultrasound showing massive diffuse hemorrhagic retinal detachment.
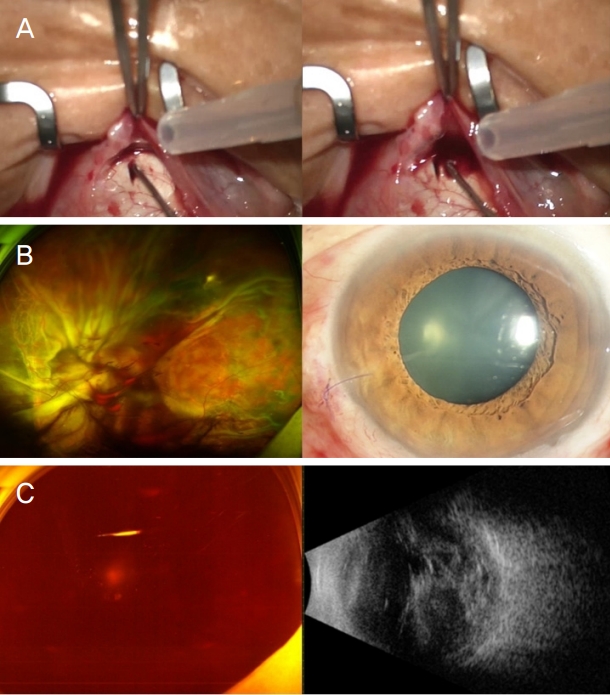
(A) A massive amount of dark blood and subretinal fluid were drained through the sclectomy site. (B) Fundus photograph and slit lamp photograph 1 day after the drainage of blood through the sclectomy site. Slit lamp photograph showing that the anterior chamber was reformed. (C) Fundus photograph and B-scan ultrasound showing massive vitreous hemorrhage 2 weeks after the operation.
고 찰
평균 연령이 증가함에 따라 삼출성 황반변성 환자의 증가와 그에 따른 항혈관내피성장인자 유리체강내 주입술은 증가하고 있으며 망막색소상피파열에 대한 빈도가 늘어나고 있다. 망막색소상피파열은 접선력에 의해 망막색소상피층이 분열이 일어나는 것으로 유리체강내 항혈관내피성장인자 주입술 후 합병증으로 0.06-27%에서 발생하고 자연경과에서 발생하는 경우보다 유발률이 높은 것으로 알려져 있다[7]. 항혈관내피성장인자 유리체강내 주입술 후 망막색소상피파열이 발생하기까지의 기간은 자연 경과나 광역학 치료 후 발생까지의 시간에 비해 주사 1-3개월 후로 이른 시기에 발생하는 것으로 알려져 있다[8]. 본 증례에서도 항혈관내피성장인자 유리체강내 주입술 1차 주사 2주 후에 망막색소상피파열이 관찰되었고, 2차 주사 4주 후에 추가적인 망막색소상피파열이 발생하였다.
Cunningham Jr et al [9]은 망막상피세포박리의 높이가 400 μm인 경우, 주사 간격이 4.5개월보다 짧은 경우, 미세파열이 관찰되는 경우, 망막하 분열이 보이는 경우, 섬유혈관성 망막색소상피박리가 동반된 경우, 이전 광역학 치료 과거력이 있는 경우를 위험인자로 보고 위험인자가 증가하는 경우에는 항혈관내피성장인자 유리체강내 주입술을 중단하고 1, 2주 후 재평가하라고 권고하고 있다. Rachitskaya and Goldhardt [10]은 반대편 눈에 망막색소상피파열이 있었던 경우, 망막색소상피박리 직경과 높이가 큰 경우, 주사 간격이 4.5개월보다 짧은 경우, 망막하액이 많은 경우를 위험인자로 보고하였다. 본 증례에서 망막색소상피박리의 높이가 1,045 μm, 직경은 5,645 μm로 파열 위험도가 높으며, 이중 망막색소상피파열은 1차 주사 후 유발된 망막색소상피파열에 전단력의 방향으로 수축력이 발생하면서 동심원 형태의 추가적인 망막색소상피파열이 발생한 것으로 생각된다.
2차 주사 4개월 후 망막하출혈이 증가하고 및 3차 주사 3개월 후 대량의 망막하출혈이 발생하였는데 이는 환자가 평소 아스피린을 복용한 기왕력으로 출혈 요인의 증가 및 유리체강내 항혈관내피성장인자 주입술 후 아주 드물게 발생할 수 있는 합병증으로 추정할 수 있다[11]. 고령, 고혈압, 당뇨, 고도근시 등의 환자들은 손상되기 쉬운 혈관구조를 가지고 있으며, 혈액질환, 항응고제, 항혈소판 약제를 사용하는 경우 지혈이 잘되지 않아 결막하 출혈부터 망막 및 맥락막 거대 출혈까지 발생할 수 있다[12]. 본 증례에서 출혈성 망막 및 맥락막박리와 함께 발생한 급성폐쇄각발작은 박리된 망막 및 맥락막하 출혈에 의해 수정체와 홍채가 앞쪽으로 이동하면서 갑자기 앞방각이 좁아지면서 발생한 것으로 생각된다[13,14]. 황반변성에서 자연 발생한 출혈망막박리로 인한 급성폐쇄각녹내장의 안압상승의 치료에 안압하강제는 효과가 떨어지는 것으로 알려져 있으며, 심한 안통을 치료하기 위해 눈뒤 알코올 주입술, 섬모체파괴술, 안구적출술이 보고되었으며 공막절개술 후 혈종 제거를 권고하고 있다[12]. 본원에서도 공막절개술을 통한 맥락막 천자술로 출혈 및 망막하액 및 망막하 출혈 외배액술을 시행하였고, 수술 1일째 안압 11 mmHg로 감소하였다. 이는 수정체와 홍채면이 원위치로 오면서 전방각폐쇄가 완화되고 전방이 형성되었기 때문이다.
망막색소상피박리가 동반된 삼출성 황반변성 환자에게 유리체강내 항혈관내피성장인자 주입술을 시행 후 발생한 이중 망막색소상피파열은 드문 것으로 알려져 있다. 환자가 망막색소상피파열의 위험인자를 갖고 있다면 더욱 주의해서 항혈관내피성장인자 주입술을 고려해야 하며, 치료 전 환자에게 충분한 설명이 필요할 것으로 생각된다. 자연 발생한 출혈망막박리 후 폐쇄각녹내장으로 실명하거나 안구제거술을 시행한 예가 드물게 보고된 바가 있다. 항혈전제 같은 약물 복용력이 있는 경우 안내 출혈 가능성이 있음을 고려하고 환자 치료 계획에 염두에 두어야 한다. 이중 망막색소상피파열이 발생한 환자에서 출혈망막박리와 급성폐쇄각발작으로 심한 시력소실을 초래한 증례는 국내에서 아직 보고된 바가 없다. 저자들은 유리체강내 항혈관내 피성장인자 주입술 치료 후 이중 망막색소상피파열 및 유리체출혈, 출혈망막박리로 인한 안압상승을 경험하고 치료하였다. 1차 주사 후 유발된 망막색소상피파열에 전단력의 방향으로 수축력이 발생하면서 동심원 형태의 추가적인 망막색소상피파열이 발생한 것으로 볼 때, 환자의 신생혈관막과 망막색소상피의 견인력이 강한 특성으로 주변의 혈관성 조직을 강하게 수축시킬 수 있는 기전이 작용하지 않았을까 생각이 된다. 이러한 주변의 혈관성 조직을 수축시키는 기전 및 정상적인 지혈 작용이 작동하지 못했을 출혈성 위험 인자가 있어 출혈성 맥락막 및 망막박리가 발생했을 가능성이 있었을 수 있다고 볼 수 있다. 하지만 본 드문 증례는 두 발생 질환에 대하여 관련성이나 인과 관계를 이야기하기에는 제한점이 있다. 그럼에도 불구하고 본 증례를 통해서 흔히 시행하는 유리체강내 항혈관내피성장인자 주입술에서 환자의 과거력, 망막색소상피의 높이나 직경 등 중요한 빛간섭단층촬영 소견의 망막색소상피파열의 발생 위험에 관한 주의를 기울이는 것에 대한 교훈을 얻을 수 있을 것으로 생각된다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
최유진 / Yu-Jin Choi
경상대학교 의과대학 안과학교실
Department of Ophthalmology, Gyeongsang National University School of Medicine
