전체각막곡률측정법과 표준각막곡률측정법을 이용한 인공수정체도수 예측의 정확도 비교
Accuracy of Intraocular Lens Power Calculations Based on Total and Standard Keratometry
Article information
Abstract
목적
Barrett Universal II 공식과 Barrett Toric Calculator에 전체각막곡률측정법과 표준각막곡률측정법을 적용하였을 때의 굴절예측정확도를 비교해보고자 하였다.
대상과 방법
백내장수술을 위해 본원을 내원한 환자 111명 111안을 대상으로 하였다. 수술 전 IOL Master 700® (Carl Zeiss Meditech AG, Jena, Germany)으로 Barrett Universal II 공식 또는 Barrett Toric Calculator를 사용한 굴절예측치와 수술 후의 현성굴절검사값을 이용하여 평균절대오차를 구하였다. 난시교정인공수정체를 넣은 대상 중 각막후면난시가 0.3 diopters (D)보다 큰 그룹을 분류하여 두 방법의 평균절대오차를 비교했다.
결과
Barrett Universal II 공식, Barrett Toric Calculator의 경우 구면렌즈대응치에 대해 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차의 차이는 각각 0.021 ± 0.102 D (p=0.65), 0.015 ± 0.121 D (p=0.80)였다. 난시교정인공수정체를 넣은 대상 중 후면각막난시가 0.3 D보다 큰 경우 구면렌즈대응치와 난시에 대한 평균절대오차 차이는 각각 -0.020 ± 0.107 D (p=0.70), -0.023 ± 0.055 D (p=0.50)였다.
결론
전체각막곡률측정법은 표준각막곡률측정법과 비슷한 굴절예측 결과를 보였고, 난시교정인공수정체를 삽입했을 때 후면각막난시가 큰 경우에도 전체각막곡률측정법이 표준각막곡률측정법에 비해 통계적인 차이를 보이지 않았다.
Trans Abstract
Purpose
To compare the accuracy of standard and total keratometry data obtained using the Barrett Universal II and Barrett Toric Calculator.
Methods
In total, 111 eyes of 111 patients who visited our hospital for cataract surgery from February 2019 to September 2019 were included in this study. Total keratometry and standard keratometry data were obtained using the Barrett Universal II and the Barrett Toric Calculator; mean absolute errors were derived by using preoperative IOL Master 700® (Carl Zeiss Meditech AG, Jena, Germany) data and 2-month postoperative manifest refraction data. The mean absolute errors of the two methods were compared in terms of a posterior corneal astigmatism greater than 0.3 diopter (D) in patients fitted with Toric intraocular lenses.
Results
Using the Barrett Universal II formula, the mean absolute error spherical equivalent difference between total keratometry and standard keratometry was 0.021 ± 0.102 D (p = 0.65) when the Barrett Toric Calculator was used. The mean absolute error differences between the two methods were 0.015 ± 0.121 D for the spherical equivalent (p = 0.80) and 0.005 ± 0.870 D for the cylinder measurement (p = 0.94). In terms of a posterior corneal astigmatism greater than 0.3 D, the mean absolute error spherical equivalent and cylinder measurement differences were -0.020 ± 0.107 D (p = 0.70) and -0.023 ± 0.055 D (p = 0.50) in patients fitted with Toric intraocular lenses.
Conclusions
The total keratometry method, which directly measures posterior corneal curvature, yields data comparable to those of the standard keratometry method. When the posterior corneal astigmatism was greater than 0.3 D, we found no significant difference between the total keratometry and standard keratometry data of patients fitted with Toric intraocular lenses.
백내장수술은 국내에서 가장 많이 시행되는 수술 중 하나이며, 고령 인구가 증가함에 따라서 점차 증가하는 추세에 있다. 백내장수술 후 안구 내에 삽입되는 인공수정체의 도수를 정하는 일은 환자의 시력에 많은 영향을 끼치는 중요한 과정이며, 백내장수술이 단순히 병을 치료하는 수술로 인식되던 과거에 비해 좋은 시력을 얻기 위한 시력교정수술의 시대로 접어들게 되면서 더욱 부각되고 있다. 백내장수술을 받는 환자들의 특성을 분석한 여러 연구에서 수술 전 각막난시가 1.25 diopter (D) 이상인 환자가 20-30%에 달한다는 보고와[1,2] 1-3 D 이상의 각막난시가 15-29%에 달한다는 보고[3,4] 등이 있으며, 이를 교정하기 위해 여러 방법에 관한 연구들이 있으며, 그중 하나인 난시교정인공수정체도 많이 사용되고 있다. 기존에 난시교정인공수정체를 삽입하기 위해 각막난시를 측정하는 방법으로 각막의 전면부만 고려하는 표준각막곡률측정법(standard keratometry, K)을 많이 사용했으나, 수술 후 난시가 과교정되거나 저교정되는 일이 발생했다[5-10]. 이에 따라 최근에는 각막의 전면부와 더불어 후면부와 각막두께를 함께 고려하는 전체각막곡률측정법(total keratometry, TK) 사용의 필요성이 대두되었고, 현재 몇몇 인공수정체도수 결정 공식들이 전체각막곡률측정법을 이용하고 있다. 여러 장비들이 각막후면을 측정하기 위해 개발되었지만, 안축장 같은 생체계측치를 측정하지 못하거나 측정한 여러 계측치들로 인공수정체도수를 계산하지 못한다는 단점이 있었다. 하지만 IOL Master 700® (Carl Zeiss Meditech AG, Jena, Germany)은 이러한 단점을 보완한 장비로, 텔레센트릭 각막곡률측정방식과 파장가변광원 빛간섭단층촬영 방식을 이용하여 각막전면과 후면을 포함한 여러 생체계측치를 측정하여 인공수정체도수 계산까지 하나의 장비로 실행할 수 있게 고안되었다[11]. 본 연구에서 저자들은 IOL Master 700®을 사용하여 새로운 전체각막곡률측정법의 정확도를 파악해보기 위해 기존의 표준각막곡률측정법을 이용한 공식과 비교했다. 그리고 후면각막난시가 평균인 0.3 D보다 큰 집단을 세분하여 전체각막곡률측정법과 표준각막곡률측정법의 정확도를 비교해보았다.
대상과 방법
2019년 2월부터 2019년 12월까지 백내장수술을 위해 본원을 내원하여 수정체유화술 및 인공수정체삽입술을 시행받은 환자를 대상으로 연구를 진행했다. 수술은 1명의 술자(J.Y.K)에 의해 진행되었으며, 수술 후 두 달까지 추적 관찰이 가능했던 환자들을 후향적으로 의무기록을 분석하였다. 양안을 수술한 환자의 경우 연구에 포함시킬 눈을 무작위로 선택하였다. 각막혼탁이나 심한 백내장으로 인해 굴절률이나 각막곡률 측정이 불가능한 환자나 술 후 시력에 영향을 줄 수 있는 각막질환이나 망막질환, 익상편수술의 과거력, 녹내장이나 외상의 과거력이 있던 환자와 수술 중 후 낭파열과 같은 합병증이 발생한 경우는 본 연구 대상에서 제외하였다.
모든 대상 환자들은 백내장수술 시행 전에 세극등검사, 나안시력, 최대교정시력, 안압검사, 자동굴절각막곡률계, 현성굴절검사, 안저검사, 각막형태검사를 시행했으며, IOL Master 700®을 이용하여 전체각막곡률, 표준각막곡률, 안축장, 전방깊이, 수정체두께, 각막두께 그리고 각막직경을 측정하였으며, 이를 바탕으로 인공수정체도수 계산을 시행하였다. 인공수정체는 Acrysof IOL SN60AT® (Alcon Laboratories Inc., Fort Worth, TX, USA)를 사용하였으며 난시교정인공수정체는 Acrysof Toric IOL® (Alcon Laboratories Inc., Fort Worth, TX, USA)를 사용하였고, 인공수정체도수계산 공식은 IOL Master 700®에 포함되어 있는 Barrett Universal II, Barret TK Universal II를 사용하였고, 각막난시가 0.75 D 이상인 환자들의 경우 난시교정인공수정체삽입을 위해 Barrett Toric calculator, Barrett TK Toric calculator를 사용하였다.
백내장수술은 2.2 mm 너비로 각막이측절개를 시행하고 Infinity vision system® (Alcon Laboratories Inc., Fort Worth, TX, USA)과 OZilTM torsional handpiece (Alcon Laboratories Inc., Fort Worth, TX, USA)를 이용하여 수정체유화술을 시행하였다. 인공수정체를 낭 속에 삽입한 후 전방과 낭 속의 모든 점탄물질을 제거하였고, 각막봉합은 시행하지 않았다. 난시교정인공수정체를 삽입하는 경우에는 백내장수술 전 환자를 정위로 앉혀놓고 환자의 머리가 기울어지지 않았는지 확인 후 30게이지 바늘과 마킹펜을 이용하여 각막윤부 3시와 9시 방향에 표시를 하였다. 그 후 수술실에서 환자가 누운 상태에서 기존에 표시한 위치를 기준으로 Toric axis marker를 이용하여 각막에 목표 난시축을 표시하였다. 난시교정인공수정체를 낭 속에 삽입한 후 전방과 낭 속의 모든 점탄물질을 제거하였고 인공수정체를 회전시켜 미리 표시해둔 위치에 평행하게 위치시켰다. 각막봉합은 시행하지않고 수술을 종료했다. 수술 종료 이후 항생제 점안액(0.5% Moxifloxacin, Vigamox®; Novartis, East Hanover, NJ, USA)과 스테로이드 점안액(1% Prednisolone acetate, Prednilone®; Daewoo pharm, Seoul, Korea)을 점안하였다.
본 연구에 사용된 통계 분석은 SPSS 18.0 for Windows(SPSS Inc., Chicago, IL, USA)를 이용하였으며, 기술통계를 사용하여 대상의 수술 전 굴절이상과 전안부계측치에 대해 평균, 표준편차, 중앙값 그리고 범위를 계산하였다. 전체각막곡률측정법과 표준각막곡률측정법 각각의 평균절대오차가 어느 방법을 적용했을 때 더 큰지 짝비교를 통해 확인하였다. Independent-sample t-test를 이용하여 각 공식에서 전체각막곡률측정법을 사용한 수술 후 굴절 예측치와 수술 후 현성굴절검사의 평균절대오차의 차이와 표준각막곡률측정법을 사용한 수술 후 굴절 예측치와 수술 후 현성굴절검사의 평균절대오차의 차이를 비교했다. Bland-Altman plot을 사용하여 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차의 차이를 계산하였으며, 평균차이 ± 1.96 × 표준편차의 방법으로 95% 일치한계값들을 계산하였다.
난시 분석은 Power vector 방법을 이용하여 Cartesian astigmatism (J0)과 Oblique astigmatism (J45)을 구하였다. 수술 전과 수술 2달 후의 현성굴절검사값을 이용하였으며 다음 수식에 대입하여 계산하였다(S는 구면치, C는 난시, α는 난시의 축을 의미한다).
J0 = (-C/2)cos(2α)
J45 = (-C/2)sin(2α)
IOL Master 700®을 사용하여 직접 측정한 후면각막난시가 0.3보다 큰 군에서 Power vector 분석을 사용하여 계산한 수술 전과 후의 J0, J45값에 대해서는 Wilcoxon signed rank test를 통하여 차이를 분석하였다. p<0.05인 경우 통계적으로 유의한 것으로 간주하였으며, p값은 소수점 셋째자리에서 반올림하여 소수점 둘째자리까지 표시하였다. 본 연구에 사용된 그래프는 SPSS 18.0 for Windows와 GraphPad Prism 5 (GraphPad Software, San Diego, CA, USA)를 사용하여 작성하였다. 본 연구는 임상시험심사위원회(institutional review board, IRB)의 승인 아래 진행되었다(IRB 승인 번호: 202002-001-01).
결 과
총 111명 111안의 환자를 대상으로 하였으며, 남성은 53명, 여성은 58명, 우안은 57안, 좌안은 54안이었다. 평균연령은 68.15 ± 10.23이었으며 그 외의 특성은 다음과 같다(Table 1).
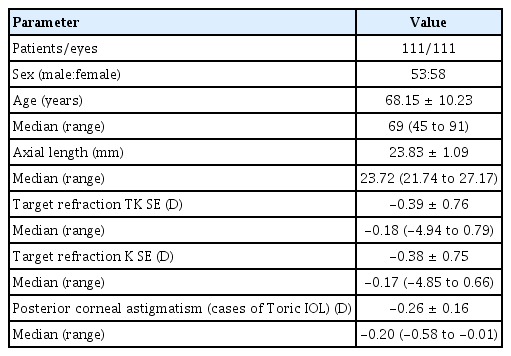
Preoperative characteristics of patients
Barrett Universal II 공식에 전체각막곡률측정법과 표준각막곡률측정법을 적용하여 구면렌즈대응치의 평균절대오차를 계산하였을 때(Table 2), 전체각막곡률측정법의 경우 0.5 D, 0.75 D, 1 D 이내의 차이를 보이는 경우가 각각 88.9%, 90.5%, 96.8%였고, 표준각막곡률측정법의 경우 0.5 D, 0.75 D, 1 D 이내의 차이를 보이는 경우가 각각 87.3%, 95.2%, 96.8%였다(Fig. 1). 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차 차이의 평균은 0.021 D였다(Table 3, Fig. 2A). 짝비교를 시행하였을 때 전체각막곡률측정법의 평균절대오차가 표준각막곡률측정법의 평균절대오차보다 큰 경우가 더 많았다(TK=32, K=30, same value=1) (Fig. 3A). 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차를 비교해보았을 때 통계적으로 유의한 차이를 보이지 않았다(p=0.65).
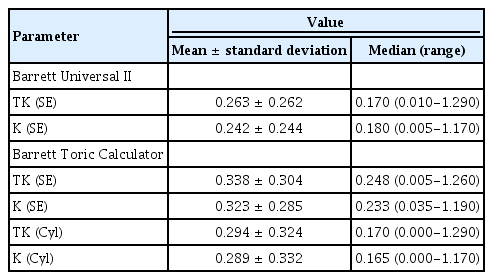
Mean absolute errors (diopters) in spherical equivalent and cylinder between TK and K using each IOL calculation formulas
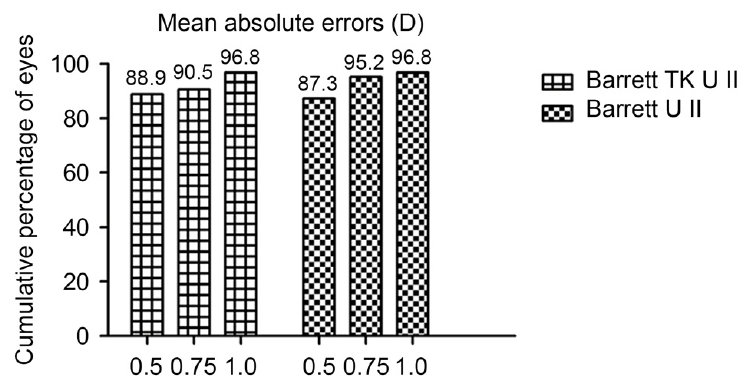
Cumulative percentage of eyes within the specified range of mean absolute errors in spherical equivalent for the Barrett total keratometry Universal II and Barrett Universal II. D = diopters; TK = total keratometry.
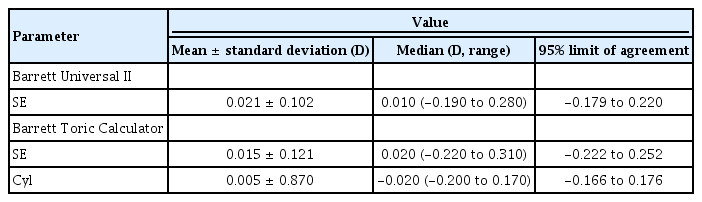
Differences of mean absolute error (diopters) in spherical equivalent and cylinder between TK and K (TK-K) using each IOL calculation formulas
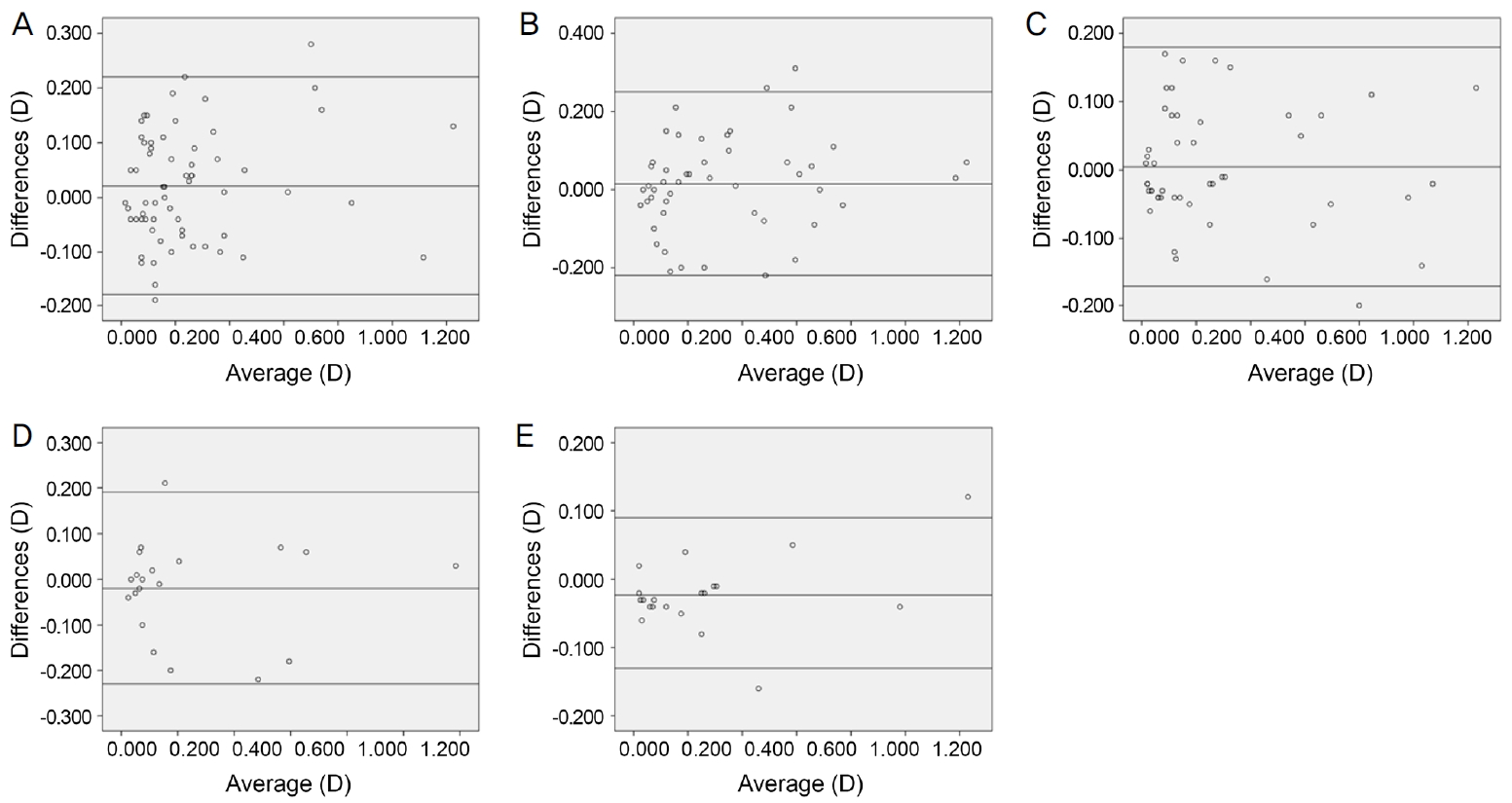
Bland-Altman plots of differences in mean absolute error between total keratometry and standard keratometry (TK-K). (A) Spherical equivalent (SE) calculated with the Barrett Universal II formula. (B) SE calculated with the Barrett Toric Calculator. (C) Cylinder calculated with the Barrett Toric Calculator. (D) SE calculated with the Barrett Toric Calculator in case of posterior corneal astigmatism greater than 0.3 D. (E) Cylinder calculated with the Barrett Toric Calculator in case of posterior corneal astigmatism greater than 0.3 D.
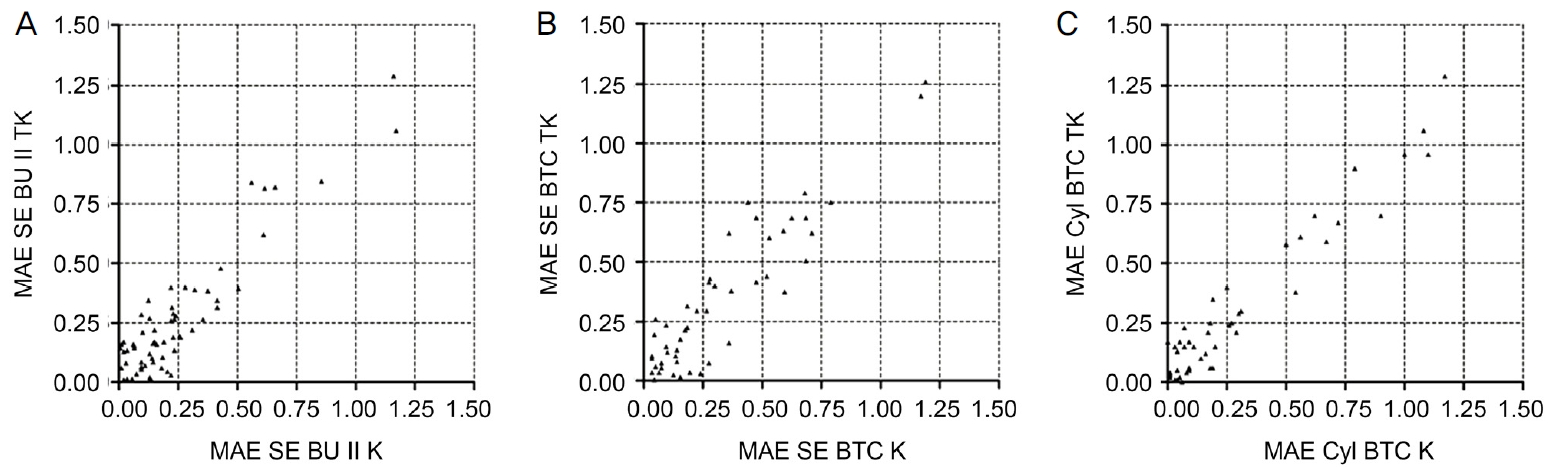
Pairwise comparison of mean absolute error (MAE) from total keratometry (TK) and standard keratometry (K). (A) MAE of spherical equivalent (SE) with the Barrett Universal (BU) II. (B) MAE of SE with the Barrett Toric Calculator (BTC). (C) MAE of cylinder (Cyl) with the BTC.
Barrett Toric Calculator에 전체각막곡률측정법과 표준각막곡률측정법을 적용하여 구면렌즈대응치의 평균절대오차를 계산하였을 때(Table 2), 전체각막곡률측정법의 경우 0.5 D, 0.75 D, 1 D 이내의 차이를 보이는 경우는 각각 72.9%, 89.6%, 95.8%였고, 표준각막곡률측정법의 경우 0.5 D, 0.75 D, 1 D 이내의 차이를 보이는 경우가 각각 각각 75%, 91.2%, 95.8%였다(Fig. 4). 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차 차이의 평균은 0.015 D였다(Table 3, Fig. 2B). 짝비교를 시행하였을 때 전체각막곡률측정법의 평균절대오차가 표준각막곡률측정법의 평균절대오차보다 큰 경우가 더 많았다(TK=27, K=18, same value=3) (Fig. 3B). 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차를 비교해보았을 때 통계적으로 유의한 차이를 보이지않았다(p=0.80). 두 방법을 적용하여 난시의 평균절대오차를 계산하였을 때(Table 2), 전체각막곡률측정법의 경우 0.5 D, 0.75 D, 1 D 이내의 차이를 보이는 경우는 각각 77.1%, 89.6%, 95.8%였고, 표준각막곡률측정법의 경우 0.5 D, 0.75 D, 1 D 이내의 차이를 보이는 경우는 각각 75%, 87.5%, 91.7%였다(Fig. 4). 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차 차이의 평균은 0.005 D였다(Table 3, Fig. 2C). 짝비교를 시행하였을 때 전체각막곡률측정법의 평균절대오차가 표준각막곡률측정법의 평균절대오차보다 큰 경우가 더 적었다(TK=21, K=27) (Fig. 3C). 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차를 비교해보았을 때 통계적으로 유의한 차이를 보이지 않았다(p=0.94).

Cumulative percentage of eyes within the specified range of mean absolute errors in spherical equivalent and cylinder for the Barrett total keratometry Toric Calculator and Barrett Toric Calculator. D = diopters; TK = total keratometry; TC = toric calculator; SE = spherical equivalent; Cyl = cylinder.
Barrett Toric Calculator를 사용하여 48명의 난시교정인 공수정체를 삽입한 환자 중 후면각막난시가 0.3 D보다 큰 20명의 환자들을 따로 분류하여 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차에 대해 짝비교를 시행하였을 때, 구면렌즈대응치의 경우 전체각막곡률측정법의 평균절대오차가 표준각막곡률측정법의 절대오차보다 큰 경우가 적었으며(TK=8, K=10, same value=2), 난시의 경우에도 마찬가지였다(TK=4, K=16). 전체각막곡률측정법과 표준각막곡률측정법의 구면렌즈대응치와 난시의 평균절대오차 차이의 평균은 각각 -0.020 D, -0.023 D였다(Fig. 2D, E). 전체각막곡률측정법과 표준각막곡률측정법으로 구면렌즈대응치의 평균절대오차를 비교했을 때 각각의 평균과 표준편차는 0.235 ± 0.304 D, 0.255 ± 0.307 D로 전체각막곡률측정법이 더 낮은 평균절대오차를 보였으나 통계적으로 유의한 차이를 보이지 않았고(p=0.70), 난시의 평균절대오차를 비교했을 때 각각의 평균과 표준편차는 0.261 ± 0.338 D, 0.283 ± 0.316 D로 전체각막곡률측정법이 더 낮은 평균절대오차를 보였으나 통계적으로 유의한 차이를 보이지 않았다(p=0.50) (Table 4). 그리고 수술 전과 후에 power vector analysis를 이용한 난시를 비교하였을 때 J0는 수술 전 -0.656 ± 0.595 D에서 수술 후 0.018 ± 0.102 D로 통계적으로 유의한 변화를 보이지 않았으나(p=0.63), J45는 수술 전 0.372 ± 0.763 D에서 수술 후 -0.037 ± 0.271 D로 통계적으로 유의한 변화를 보였다(p=0.03) (Fig. 5).

Mean absolute errors (D) in spherical equivalent and cylinder between TK and K using Barrett Toric Calculator in case of posterior corneal astigmatism greater than 0.3 D

Scatter plots of cases of posterior corneal astigmatism greater than 0.3 diopters (D) of J0 and J45 vectors of preoperative (A) and postoperative (B) astigmatism. Calculated by power vector analysis.
고 찰
표준각막곡률측정법을 사용하여 인공수정체도수를 계산하게 되는 경우 각막전면의 곡률은 직접 측정하고 각막후면의 곡률은 정해진 비율로 계산을 하여 예측하게 된다[10]. 그리고 이는 본 연구에서 사용한 Barrett Universal II 공식과 난시교정인공수정체를 삽입하기 위한 공식이지만 구면 렌즈대응치를 구하기 위해 Barrett Universal II 공식을 사용하는 Barrett Toric Calculator의 경우에도 마찬가지이다[12]. 하지만 실제 각막의 전체굴절력은 각막전면과 각막후면의 곡률과 각막두께에 영향을 받기 때문에 각막후면을 반드시 고려해야 한다[13]. 그리고 난시교정인공수정체를 삽입하는 경우에도 각막후면을 고려하지 않았다가 수술 후 큰 굴절오차가 발생하는 경우가 보고되었다[14,15].
Fabian and Wehner [13]는 Barrett Universal II 공식으로 표준각막곡률측정법의 평균절대오차에서 전체각막곡률측정법의 평균절대오차를 뺐을 때, 0.016 ± 0.113 D로 전체각막곡률측정법이 더 정확하다고 보고하였고, Srivannaboon and Chirapapaisan [16]도 같은 공식으로 전체각막곡률측정법의 평균절대오차에서 표준각막곡률측정법의 평균절대오차를 뺐을 때 -0.05 D로 전체각막곡률측정법이 더 정확하다고 보고하였다. 본 연구에서 같은 공식으로 전체각막곡률측정법의 평균절대오차에서 표준각막곡률측정법의 평균절대오차를 뺐을 때의 결과는 0.021 ± 0.102 D로 전체각막곡률측정법의 정확도가 낮았으나, 두 방법을 비교해보았을 때 통계적으로 유의하지 않았다(p=0.65).
난시가 있어 난시교정인공수정체를 삽입한 경우에 대해서 Fabian and Wehner [13]은 Barrett Toric Calculator 공식을 사용하여 난시에 대한 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차의 차이가 0.020 ± 0.148 D임을 확인하고 전체각막곡률측정법이 더 정확하다고 보고하였고, Reitblat et al [9]은 난시교정인공수정체를 삽입할 때 후면각막난시를 고려했을 경우 예측되는 잔여난시가 0.47 D에서 0.22 D로 감소된다고 보고하였고, 이를 위해 샤임플러그 카메라로 후면각막난시를 측정하고 광저간섭반사광측 정기로 전면각막난시를 측정하는 방법을 제안하였다. 하지만 Skrzypecki et al [17]처럼 Barrett Toric Calculator를 사용하여 전체각막곡률측정법과 표준각막곡률측정법의 평균절대오차를 비교했을 때, 표준각막곡률측정법을 사용했을 때, 평균절대오차가 0.33 ± 0.15 D로 전체각막곡률측정법을 사용했을 때의 0.31 ± 0.23 D보다 크긴 했지만 통계적으로 유의한 차이를 보이지 않았다는 결과를 보고한 연구도 있다. 그리고 Ferreira et al [18,19]은 후면각막난시의 영향을 예측하는 것이 후면각막난시를 직접 측정하는 것보다 더 좋은 결과를 가져오며, 후면각막난시의 직접 측정이 예측에 비해 우세하지 않다는 두 연구를 발표한 바가 있다. 본 연구에서는 같은 공식으로 전체각막곡률측정법의 평균절대오차에서 표준각막곡률측정법의 평균절대오차를 뺐을 때, 구면렌즈대응치는 0.015 ± 0.121 D, 난시는 0.005 ± 0.870 D로 각각 전체각막곡률측정법의 정확도가 낮았으나 두 방법을 비교해보았을 때 통계적으로 유의하지 않았다(p=0.80, p=0.94).
본 연구에서 Barrett Universal II 공식과 Barrett Toric Calculator 공식에 전체각막곡률측정법과 표준각막곡률측정법을 적용하였을 때 표준각막곡률측정법이 조금 더 우세한 평균절대오차를 보였고, 짝비교에서도 전체각막곡률측정법의 평균절대오차가 표준각막곡률측정법의 평균절대오차 보다 큰 경우가 많은 경향을 보였다. 그러나 Bland-Altman plot을 시행했을 때 각 공식에서 표준각막곡률측정법과 전체각막곡률측정법의 평균절대오차 차이의 평균은 0에 매우 가깝다. 그러므로 전체각막곡률측정법에 의해 예측한 굴절예측치는 기존 방법인 표준각막곡률측정법과 비슷한 정확도를 보였다고 할 수 있다. 그리고 Barrett Universal II 공식과 Barrett Toric Calculator에서 두 가지 방법을 이용한 평균절대오차를 비교해보았을 때 통계적으로 유의한 차이를 보이지 않았으므로 각 공식에서 전체각막곡률측정법은 표준각막곡률측정법을 사용하는 것과 대등하다고 할 수 있다. 그리고 본 연구는 435명 715안을 대상으로 후면각막난시를 분석 후 후면각막난시의 평균이 0.3 D임을 밝힌 Koch et al [8]의 연구 결과를 참고하여, IOL Master 700® 장비로 직접 측정한 후면각막난시가 평균으로 알려진 0.3 D보다 큰 경우의 전체각막곡률측정법과 표준각막곡률측정법을 비교해 본 최초의 연구로, Barrett Universal II 공식과 Barrett Toric Calculator 공식을 사용하여 두 방법 간 평균절대오차를 비교했을 때 통계적으로 유의한 차이를 보이지는 않았지만, Barrett Toric Calculator 공식을 사용한 전체 군에서 표준각막곡률측정법이 조금 더 정확하게 예측하는 경향을 보인 반면에, 후면각막난시가 0.3 D 이상인 군에서는 통계적으로 유의하진 않았지만 전체각막곡률측정법의 평균절대오차가 더 작았다.
전체각막곡률측정법과 표준각막곡률측정법을 비교한 여러 연구가 있었고, 본 연구는 그중에서 Skrzypecki et al [17]와 비슷한 결과를 보였다. 그리고 후면각막난시가 큰 경우에는 통계적으로 유의하지는 않더라도 전체각막곡률측정법의 평균절대오차가 표준각막곡률측정법에 대해서 우세했기 때문에, 후면각막난시가 큰 환자에게 있어서 전체각막곡률측정법을 이용한 인공수정체도수 계산이 조금 더 높은 정확성을 보일 수 있다고 생각되나 이에 대해서는 추가적인 연구가 필요할 것이다.
본 연구의 첫 번째 한계점은 후향적 연구라는 점이다. 전향적이었으면 조금 더 다양한 특성의 대상을 연구에 포함시켰을 수 있었을 것이다. 두 번째 한계점은 후면각막난시가 0.3 D가 넘는 대상의 수가 적다는 점이 있다. 더 많은 대상을 포함시킬 수 있었다면 본 연구에 신빙성이 더해졌을 것이며, 추후 더 많은 대상으로 한 연구가 필요하다고 생각한다.
결론적으로 Barrett Universal II 공식에서 전체각막곡률측정법과 표준각막곡률측정법으로 예측한 평균절대오차는 통계적으로 유의한 차이가 없었고, 본 연구에서 전체각막곡률측정법을 사용한 공식이 표준각막곡률측정법을 사용한 기존 공식에 뒤떨어지지 않음을 확인할 수 있었다. Barrett Toric Calculator에서 역시 전체각막곡률측정법이 표준각막곡률측정법과 유사한 정확도를 보였다. 후면각막난시가 0.3 D보다 큰 군의 경우에서 구면렌즈대응치와 난시의 평균절대오차는 전체각막곡률측정법이 표준각막곡률 측정법과 비교해서 통계적인 차이가 없음을 알 수 있었다. 본 연구에서 후면각막난시가 0.3 D보다 큰 환자의 경우에는 전체각막곡률측정법을 사용하여 인공수정체도수 계산을 시행하는 것이 표준각막곡률측정법을 사용하는 것에 비해 얻는 이점은 없었으나, 각막전면의 난시로부터 각막후면의 난시를 예측하기 힘든 원추각막과 같은 각막질환이 있거나 굴절교정수술을 받은 후의 각막의 경우에는 후면각막난시를 직접 측정하여 인공수정체도수를 계산하는 방법이 조금 더 효율적일 수 있을 것이며, 이에 대한 추가 연구가 필요할 것이다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
박세영 / Se Young Park
새빛안과병원
Saevit Eye Hospital
