방선균과 동반 감염된 침습성 진균 부비동염에 의한 안와첨증후군
Orbital Apex Syndrome Caused by Co-infection of Actinomyces with Invasive Fungal Sinusitis
Article information
Abstract
목적
세균과 진균의 동반감염에 의한 침습성 부비동염에 의해 발생한 안와첨증후군을 경험하였기에 이를 보고하고자 한다.
증례요약
87세 여자가 2주 전부터 발생한 좌안의 시력저하로 내원하였다. 과거력은 협심증과 조절되지 않는 당뇨병 병력이 있었다. 좌안 교정시력은 0.2, 안압은 정상 범위였으며, 좌안의 경한 안검하수가 관찰되었고, 외전장애가 동반되어 있었다. 조영제를 사용한 뇌 자기공명영상검사(magnetic resonance imaging)에서, 좌측 상악동의 부비동염과 날개입천장오목을 침범하는 병변이 관찰되었다. 이비인후과에서 기능내시경 부비동수술을 시행하였으며 병리조직검사에서 아스페르길루스(Aspergillus)와 방선균(Actinomyces) 동반감염을 확인하였다. 수술 후 좌안 시력은 광각무였으며, 전체눈근육마비로 진행되었다.
결론
아스페르길루스(Aspergillus)와 방선균(Actinomyces) 동반감염으로 발생한 안와첨증후군을 경험하였기에 보고하고자 한다.
Trans Abstract
Purpose
We report a case of orbital apex syndrome caused by co-infection of Actinomyces and Aspergillus invasive fungal sinusitis.
Case summary
An 87-year-old female visited our clinic for decreased visual acuity which began 2 weeks prior to her visit. She had a history of angina and uncontrolled diabetes. Her best-corrected visual acuity (BCVA) of the left eye was 0.2, the intraocular pressure was in the normal range, and mild ptosis with impaired abduction was noted. Gadolinium-enhanced brain magnetic resonance imaging showed left maxillary sinusitis and an enhanced lesion invading the pterygopalatine fossa. Functional endoscopic sinus surgery was performed by an otorhinolaryngologist. Pathology revealed co-infection with Aspergillus and Actinomyces. Her left BCVA was negative light perception despite surgery and impaired abduction progressed to total ophthalmoplegia.
Conclusions
We report a case of orbital apex syndrome caused by invasive fungal sinusitis with a rare co-infection of Actinomyces and Aspergillus.
침습성 진균 부비동염(invasive fungal sinusitis)은 50-60%에서 안와를 침범한다고 알려져 있으며, 안와 주변 구조물의 감염이 시력저하 및 안구운동장애를 동반하는 안와첨증후군(orbital apex syndrome)으로 진행할 수 있다[1,2]. 안와를 침범하는 아스페르길루스증(aspergillosis)은 매우 드문 질환으로 면역저하 환자에서 기회감염으로 흔히 발생하며, 주로 코곁굴 감염 후 발생하는데, 비침습성 아스페르길루스 감염이라도 환자의 면역기능이 떨어지면 침습성으로 변하여 문제를 일으키는 경우가 있다. 안구의 아스페르길루스 감염은 두개내로 파급될 가능성이 높아 예후가 불량하며, 중추신경계로 파급될 경우 치사율이 40-80%로 생존율이 불량하므로 질환의 신속한 진단과 적절한 치료가 필수적이다[3]. 안와를 침범하는 방선균증(actinomycosis) 또한 매우 드물게 보고되어 있으며, 동반감염된 병원균의 도움으로 질환의 전파가 가능하다[4]. 국내에서 백내장수술 후 동반된 특발안와염[5], 외상[6-9], 림프종[10,11], 점액낭종[12], 세균성 뇌막염에 의한 안와첨증후군이 보고되어 있다[6]. 국외에서 안와의 결핵균과 아스페르길루스의 동시감염이 보고된 바 있고[13], 블라스토마이세스(Blastomyces species)와 아스페르길루스의 동시감염으로 안와첨증후군이 발생하여 시력을 상실한 증례가 보고된 바 있다[14]. 또한 매우 드물게 아스페르길루스와 방선균이 동반된 폐감염 사례가 보고되어 있으나[15], 저자들은 국내/외에 처음으로 단안에 아스페르길루스와 방선균의 동반감염에 의한 침습성 진균 부비동염에 의해 발생한 안와첨증후군 1예를 경험하였기에 이를 보고하고자 한다.
증례보고
87세 여성이 내원 2주 전부터 발생한 좌안의 시력저하를 주소로 내원하였다. 과거력으로 협심증과 조절되지 않는 당뇨병을 앓고 있었으며, 2년 전 양안 백내장수술 외에 안구 주위 외상 등의 병력은 없었다. 내원 시 교정시력은 우안 0.8, 좌안 0.2였고, 안압은 양안 모두 정상 범위 내에 있었다. 양안에서 눈꺼풀처짐이 있었으나 좌안이 조금 더 심했고, 안구돌출은 명확히 관찰되지 않았다. 눈의 충혈이나 통증은 동반되지 않았다. 세극등검사와 동공반응검사, 안저검사에서 특이 소견은 없었다. 안구운동검사에서 제일안위에서 좌안 40 prism diopters (PD)의 비일치내사시가 있었고, 좌안의 -4 정도의 외전장애가 관찰되었다(Fig. 1). 초진시 시행한 안저촬영검사 및 빛간섭단층촬영검사에서는 특이 이상 소견은 관찰되지 않았다.
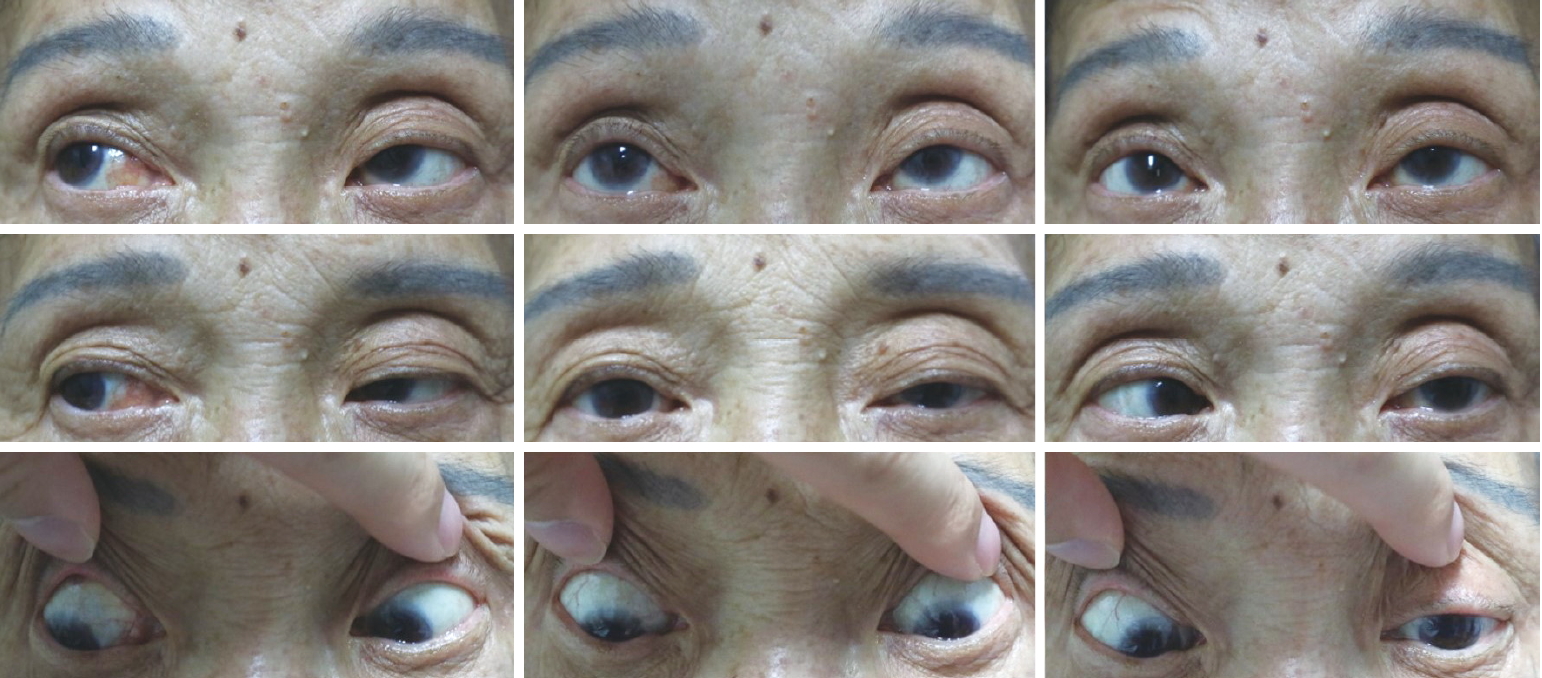
Nine-cardinal photo of the patient. The patient had 40 prism diopters of left esodeviation, and lateral gaze limitation of her left eye.
이에 외향신경마비 추정진단하에 동반된 시력저하가 있어 조영제를 사용한 뇌자기공명영상 검사를 시행하였다. 검사 결과에서 좌측의 해면정맥굴, 안와첨, 날개입천장오목을 침범하는 조영증강 병변이 관찰되었다(Fig. 2A). 영상의학과 소견에서 허혈, 종양보다는 감염에 의한 병변 가능성이 있어 뇌신경마비보다 감염성 원인이 더 의심되어 조영제를 사용한 부비동 컴퓨터단층촬영을 재시행하였다. 날개입천장오목을 침범하여 골파괴가 동반된 좌측의 상악동 부비동염이 관찰되었다(Fig. 2B, C). 이비인후과에서 전신마취하 기능내시경 부비동수술을 집도하였고, 좌측의 상악동에서 진균구(fungal ball)로 의심되는 병변에 대하여 절제생검을 시행하였다. 병리조직검사에서 아스페르길루스에 의한 진균구와 함께 있는 선상의 세균 집락 소견이 관찰되었고, Gomori Methenamine Silver 염색 결과 아스페르길루스와 합병된 방선균임을 확인하였다(Fig. 3).
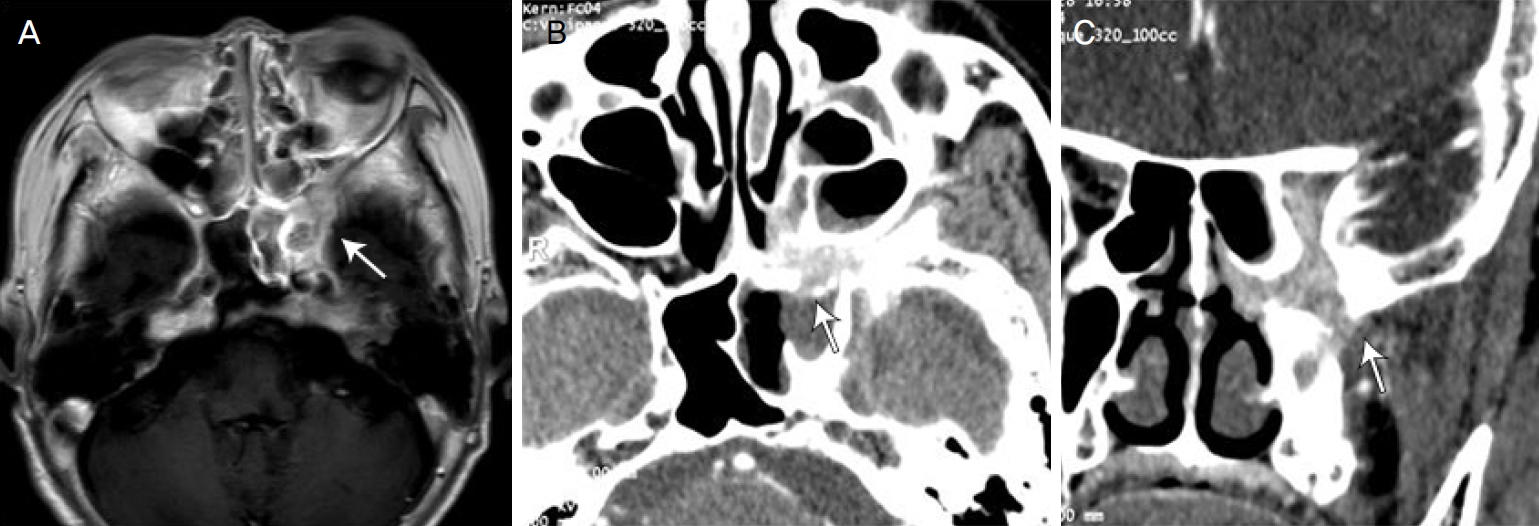
Gadolinum enhanced brain magnetic resonance imaging. T1 image shows high signal intensity lesion involving left cavernous sinus, orbital apex, and pterygopalatine fossa (arrows). (A) Ultravist enhanced paranasal sinus computed tomography. Enhancing soft tissue lesion involving left cavernous sinus, orbital apex, and pterygopalatine fossa is shown. Outbulging contour of left cavernous sinus, enhancing lesion of lesion of orbital apex with vascular congestion is seen. Sclerotic change and bony destruction of pterygoid base are demonstrated with left sphenoid sinusitis (B, C).
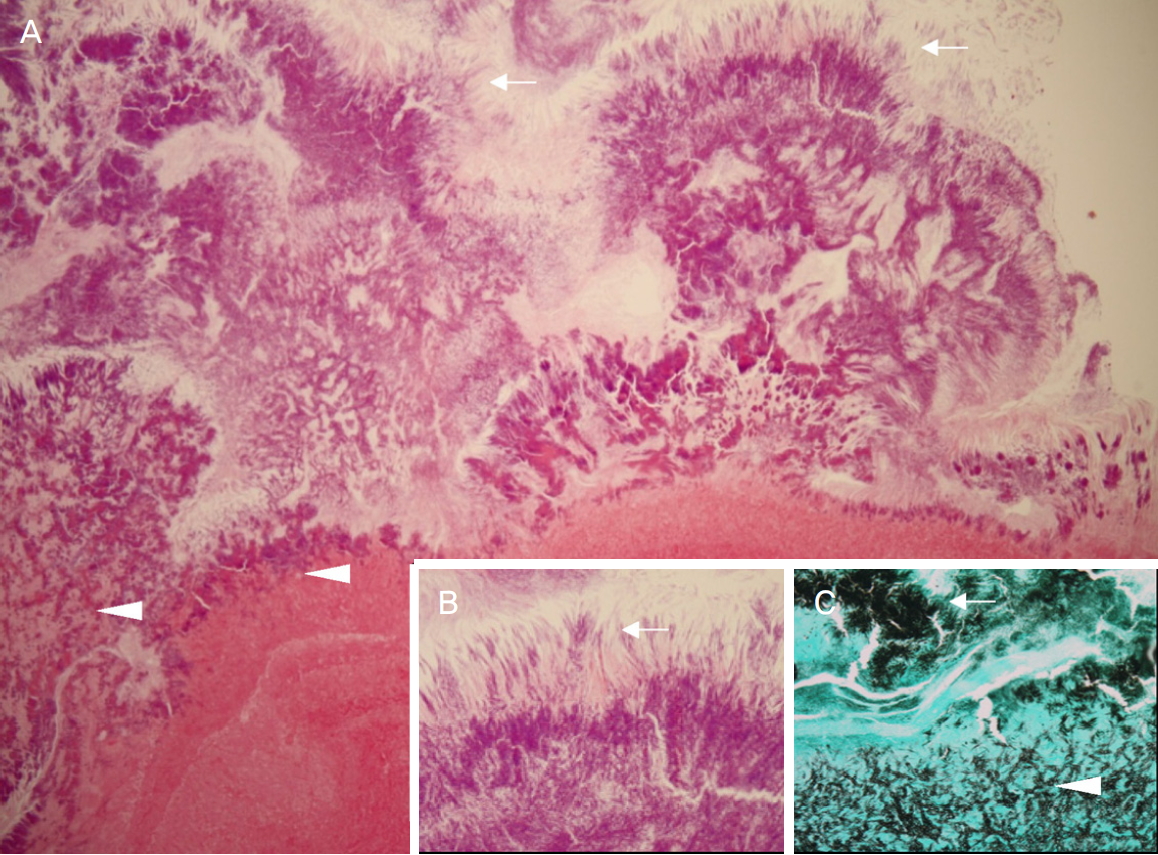
Histopathological finding of postoperative specimen. Aggregate of Actinomyces composed of filamentous bacteria (arrows) are attached to the fungus ball of Aspergillus (arrowheads) (A, B) (hematoxylin and eosin, ×40, ×200). Gomori Methenamine Silver (GMS) stain shows positive in both Actinomyces (arrow) and Aspergillus (arrowhead) (C) (GMS, ×200).
침습성 진균 부비동염 추정 진단하에 항진균제 및 항생제 치료를 시행하였다. 수술 후 2개월 뒤 내원 시 우안 교정시력 0.8, 좌안 교정시력 광각무로 감소하였다. Hertel 안구돌출계 검사에서 좌안이 우안에 비해 1 mm 돌출된 것으로 측정되었다. 좌안에 상대적 구심동공운동장애가 동반되었으며, 우안에 비해 중간 크기로 동공이 이완된 소견이 관찰되었다. 안구운동검사에서 제일안위에서 좌안의 25 PD 내사시 및 20 PD 상사시가 있었고, 전체눈근육마비로 진행되었다. 안저검사에서 좌안 시신경창백 소견이 동반되었고, 문양 시유발전위 검사에서 좌측 P100파형 관찰되지 않았다(Fig. 4).
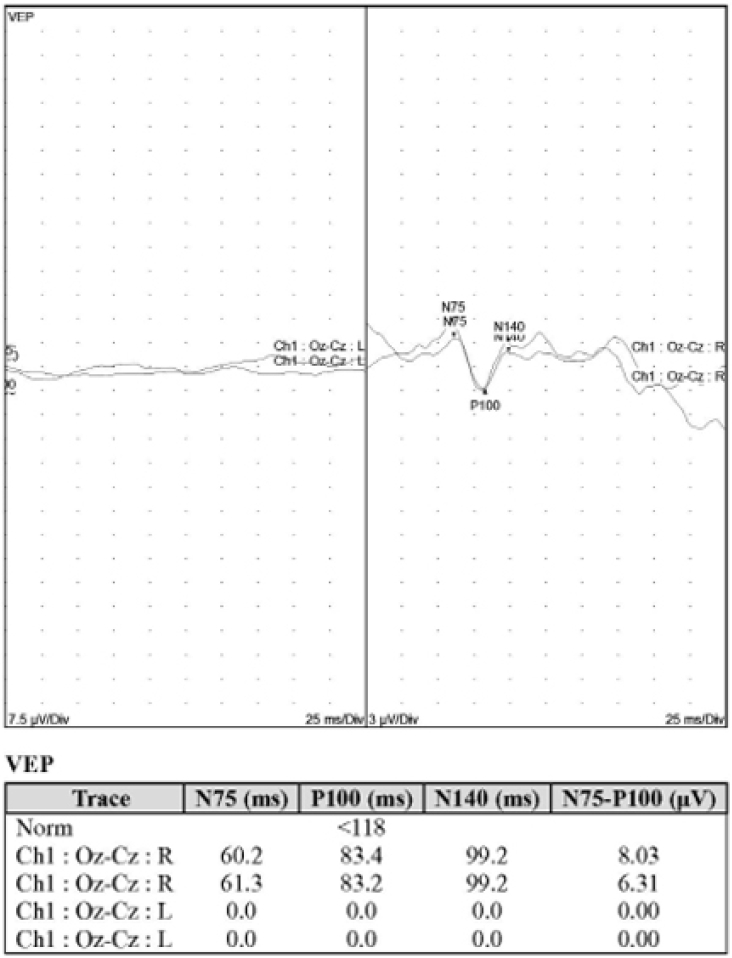
Pattern visual evoked potential (VEP) of the patient. The examination shows no P100 response on left eye.
고 찰
침습성 아스페르길루스증 안와 침범은 백혈구감소증, 장기간의 스테로이드제제 사용, 알코올 중독, 제2형 당뇨병, 혈액암, 인공삽입물이 있는 경우, 외상, 아스페르길루스에 지속적 노출, 유행지역 거주, 고령 등의 요인과 관계된 면역기능이 저하된 환자에서 주로 나타나며, 정상 면역의 환자에서도 비침습성 아스페르길루스증에서 면역저하시 침습성으로 전환되어 안와 침범을 일으킬 수 있다[1,16]. 파급 기전으로 혈관으로의 침습과 곰팡이 독소에 의한 응집괴사가 특징적이며[17], 부비동염의 경우 포자를 흡입하여 발생한다[18]. 안와내 침범시 사상판이나 안와첨을 통해 두개내로 파급이 가능하며, 해면정맥동 색전, 대뇌경색, 뇌수막염, 농양 등이 나타나고, 사망에 이를 수 있다[19]. 침습성 진균 부비동염은 안와첨증후군의 원인 중 가장 사망 위험성이 크며, 사망률이 86%까지 보고되기도 하였다[20].
안와첨은 후사골공(posterior ethmoidal foramen)과 시신경관(optic canal), 상안와열(superior orbital fissure)의 개구부 사이의 공간이며, 눈으로 가는 모든 신경과 혈관이 지나가는 통로이고, 하사근을 제외한 모든 외안근의 기시부이다[21]. 안와첨증후군은 3번 뇌신경, 4번 뇌신경, 6번 뇌신경, 5번 뇌신경의 안분지(ophthalmic division)의 기능 이상과 더불어 시신경의 손상이 동반되는 증상이 특징적이다[22]. 안구운동장애, 감각변화, 외안근 마비, 안검하수 등의 증상이 나타나는데, 이는 각각 2, 3, 4, 6번 뇌신경 기능 이상과 관련이 있다[11]. 해면정맥동 증후군(Cavernous sinus syndrome)은 5번 뇌신경의 상악분지(maxillary division)의 기능 이상까지 포함되나 시신경 손상은 없고, 상안와열 증후군(superior orbital fissure syndrome)은 안와첨증후군의 특징 중 시신경 손상이 없는 것으로 감별할 수 있다[22].
안와첨증후군의 원인 질환을 파악하기 위해서는 전산화단층촬영 및 자기공명영상 등 영상검사가 시행되어야 한다. 골절, 구후부 출혈 확인에는 전산화단층촬영이 유리하며, 종양 및 시신경 염증, 부종 등의 관찰에는 자기공명영상이 선호된다[7].
이 증례에서는 고령, 조절되지 않는 당뇨병에서 외향신경마비 추정 진단하에 뇌영상검사를 시행하지 않았다면, 초기 진단이 늦어질 가능성이 있었다. 환자의 내원시 주호소인 좌안의 시력저하와 동반된 경미한 안검하수에 대한 철저한 안과적 검사가 필수적이다. 진균성 부비동염의 안와 및 두개내 파급시 확정된 치료는 없으며, 아스페르길루스증은 혈관에 따른 파급이 가능하고, 조직의 직접적인 침윤을 통한 괴사가 가능하여 조기 진단과 함께 항진균제 치료 및 수술적 치료를 하는 것이 좋은 결과를 얻을 수 있다고 여겨진다[23].
저자들은 조절되지 않는 당뇨병 병력을 가진 고령의 환자에서 단안의 시력저하와 동반된 외전장애에서 아스페르길루스와 방선균의 동반감염에 의한 침습성 진균 부비동염에 의해 발생한 안와첨증후군을 진단하였다. 고령의 당뇨병 환자에서 비전형적인 마비사시가 나타나는 경우에는 진균과 세균에 의한 감염성 원인이 동반될 가능성을 고려해야 하며, 뇌영상검사를 반드시 적시에 시행하는 것이 중요하다고 생각된다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
윤정석 / Jung Suk Yoon
건양대학교 의과대학 안과학교실
Department of Ophthalmology, Konyang University College of Medicine
