전신 및 점안 스테로이드, 유리체절제술을 통해 호전된 브롤루시주맙 연관 망막혈관염 1예
Brolucizumab Related Retinal Vasculitis Treated with Systemic and Local Steroid, and Vitrectomy
Article information
Abstract
목적
브롤루시주맙 주사 후 발생한 안내 염증 및 망막혈관염을 전신 및 국소 스테로이드, 유리체절제술을 시행하여 치료한 1건의 증례를 보고하고자 한다.
증례요약
80세 남성이 습성 나이관련황반변성으로 2주 전 애플리버셉트에서 브롤루시주맙으로 교체 투여 후 좌안의 충혈, 통증 및 시력저하 증상이 발생해 내원하였다. 교체 투여 이전의 좌안의 최대교정시력은 0.4였고, 내원 시 좌안 최대교정시력 안전수지 10 cm로 측정되었다. 브롤루시주맙에 의한 안내 염증 및 망막혈관염을 의심해 국소 및 전신 스테로이드 치료를 받았고, 이후 유리체절제술도 시행하였다. 수술 후 환자의 증상 및 시력은 개선되었고, 나이관련황반변성 치료를 위해 항혈관내피성장인자를 추가 투여받았다. 1년 후 환자의 좌안 최대교정시력은 0.5로 측정되었으며 안내 염증 재발은 관찰되지 않고 있다.
결론
브롤루시주맙 연관 안내 염증 반응이 확인되는 경우 적극적인 치료를 하는 것이 중요하며, 양호한 망막 해부학 및 시력 결과를 얻을 수 있음을 본 증례를 통해 보고한다.
Trans Abstract
Purpose
To describe a case of retinal vasculitis that followed intravitreal brolucizumab injections and its treatment using local and systemic steroid and vitrectomy.
Case summary
An 80-year-old male diagnosed with wet age-related macular degeneration presented after experiencing redness, pain, and vision loss in his left eye following a switch in treatment from aflibercept to brolucizumab 2 weeks earlier. Before the switch, the patient’s best corrected visual acuity of the left eye was 0.4; however, on arrival at the clinic, it was finger count at 10 cm. Suspecting intraocular inflammation and retinal vasculitis caused by brolucizumab, he was treated with both local and systemic steroids and later underwent a vitrectomy. Post-surgery, the patient’s symptoms and vision improved and he received additional anti-vascular endothelial growth factor injections. One year after onset, the corrected vision of his left eye was 0.5 with no observed recurrence of intraocular inflammation.
Conclusions
When reactions related to intraocular inflammation associated with brolucizumab are identified, aggressive treatment is crucial. The present case report suggests that satisfactory anatomical and visual outcomes can be achieved.
브롤루시주맙(Beovu®, Novartis Pharma AG, Basel, Switzerland)은 최근 Food and Drug Administration에서 승인된 항혈관내피성장인자 약물로서, 나이관련황반변성 치료에 사용되고 있다.1 브롤루시주맙의 다기관 임상 연구인 HAWK과 HARRIER에 따르면, 브롤루시주맙 6 mg 주사는 애플리버셉트(Eylea®, Regeneron, Tarrytown, NY, USA)와 비교하여 시력 호전 측면에서 열등하지 않았으며, 중심망막두께 감소 및 삼출물 감소에 있어서도 뛰어난 효과를 보였다. 또한, 브롤루시주맙 투여 후 48주가 경과한 시점에서는 투여 간격을 12주로 늘릴 수 있었으며, 75% 이상의 환자들이 투여 96주째에도 12주 간격으로 투여를 진행할 수 있었다.2 이러한 임상 시험 결과로부터 브롤루시주맙 투여가 질병 관리 및 치료에 있어서 내원 불편 및 경제적 부담을 덜 수 있는 가능성을 기대하였었다. 그러나 다른 항-vascular endothelial growth factor (VEGF) 약제들과 비교하면, 브롤루시주맙의 경우 더 높은 안내 염증의 발생이 보고되고 있다.3,4
현재 브롤루시주맙은 국내에서 널리 이용되는 항VEGF 약제 중 하나로 자리잡았으나, 국내에서 브롤루시주맙 연관성 망막혈관염 및 이에 대한 치료에 관한 문헌은 제한적으로 보고되었다.5 본 증례에서 브롤루시주맙 주사 후 및 안내 염증을 경구 스테로이드 투여, 트리암시놀론 테논낭 밑 주사, 유리체절제술로 치료한 점, 안내염 치료 후 항혈관내피성장인자 주사로 유의미한 시력 호전을 거두었다는 점에서 의의가 있다. 이를 문헌 고찰과 함께 보고하고자 한다.
증례보고
2주 전 애플리버셉트에서 브롤루시주맙으로 교체 투여한 80세 남성이 1주 전부터 시작된 좌안 충혈, 통증 및 시력저하로 예약일에 앞서 내원하였다. 환자는 과거에 좌안 열아홉 차례 라니비주맙(Lucentis®, Genentech, South San Francisco, CA, USA), 여덟 차례 애플리버셉트 주사를 받았었으며, 양안 수년 전 백내장수술을 받았으며, 후두암으로 타원에서 항암 및 방사선 치료를 받았던 병력이 있었다. 수차례 8주간 정기적인 애플리버셉트 주사 및 애플리버셉트 주사 증량 치료에도 시력 개선 및 호전이 보이지 않고, 빛간섭단층촬영에서 망막내액 호전이 없어(Fig. 1A) 브롤루시주맙으로 교체 투여받았다.

Optical coherence tomography of left eye (A) before switching into brolucizumab, intraretinal fluid (yellow arrow) is observed, (B) 2 weeks after switching into brolucizumab, red arrows indicate increased subretinal fluid and blue arrow indicates subretinal pigment epithelium fluid, (C) 3 weeks after switching into brolucizumab, and 1 week after oral steroid, topical steroid, and subtenone triamcinolone injection. Subretinal fluid has disappeared however image quality is poor due due to decreased signal strength, probably due to floater, (D) 4 weeks after switching into brolucizumab and 1 week after vitrectomy. Intraretinal cyst, subretinal and sub-retinal pigment epithelium fluid have disappeared. Image quality has improved after vitrectomy.
교체 투여 이전의 좌안의 최대교정시력은 0.4였고, 내원 시 좌안 안전수지 10 cm, 좌안 안압 15 mmHg로 측정되었다. 자동 굴절률검사에서는 좌안 굴절률 값이 측정되지 않았다. 세극등현미경검사에서 좌안 결막충혈이 관찰되었고, 각막부종 및 각막후면침착물(Fig. 2) 및 전방세포가 관찰되었으며, 우안은 특이 소견이 없었다. 안저검사 결과로는 좌안 유리체부유물이 관찰되었고, 우안은 특이 소견을 보이지 않았다(Fig. 3A). 2주 전 시행한 망막 빛간섭단층촬영상 망막내액을 동반한 황반부종이 관찰되었으나(Fig. 1A), 내원일 시행한 빛간섭단층촬영상 망막내액은 감소, 망막하액 증가 소견이 관찰되었다(Fig. 1B). 망막혈관염이 의심되어 이를 감별하고자 형광안저촬영을 시행하였다. 망막동맥혈관 및 정맥혈관이 조영이 지연되었으며, 망막혈관 과형광 및 후기에서는 시신경 부위 형광물질 누출이 확인되었다(Fig. 4). 안저 소견상 브롤루시주맙과 연관된 폐쇄성 혈관염을 의심하였으나, 형광안저촬영에서 폐쇄혈관망막 병변이 관찰되지 않아 브롤루시주맙 주사 후 혈관폐쇄망막병증을 동반하지 않은 망막혈관염이 있는 경우를 의심해 치료를 시작하였다. 경구 스테로이드 30 mg 투여, 좌안 트리암시놀론(triamcinolone acetonide 40 mg/mL; Tamceton®, Hanall BioPhapma, Seoul, Korea) 테논낭밑주사 및 1% prednisolone acetate (Predforte®, Allergan Inc., Irvine, CA, USA) 안약 점안을 시작하였다.
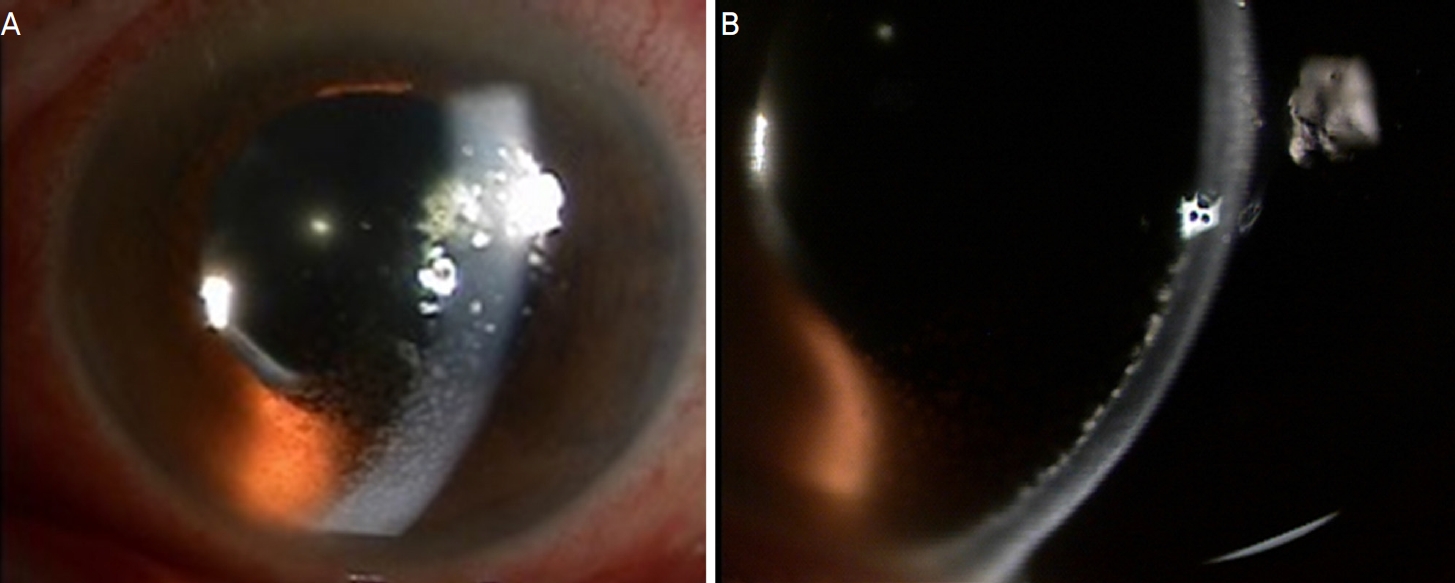
Slit-lamp photography of the left eye the initial examination (A) showing injected conjunctiva with mutton fat keratic precipitate and corneal edema. (B) representing keratic precipitate at the posterior cornea.
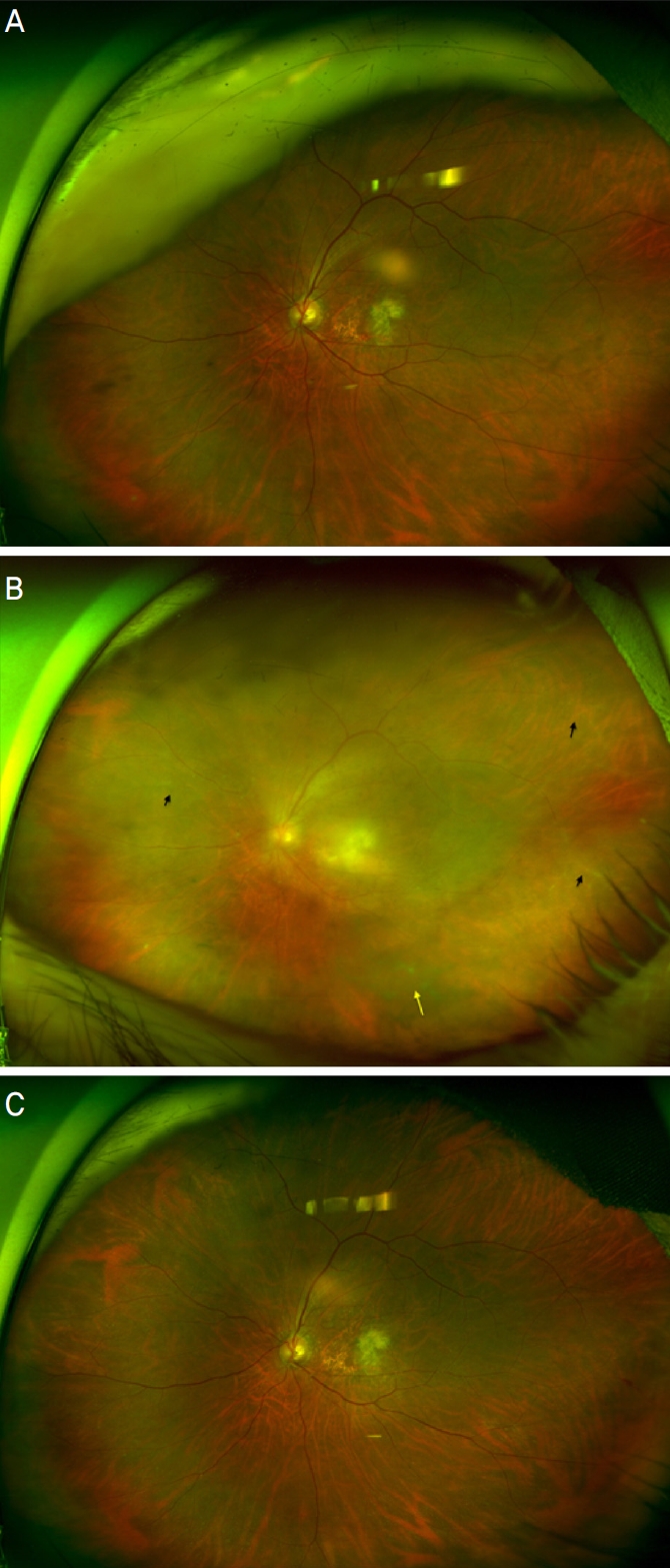
Wide fundus photo. Left eye (A) before injection of brolucizumab, (B) 2 weeks after injection of brolucizumab, suspicious retinal vessel occlusion and sheathing is apparent (black arrow). multiple vitreous debris is also found (yellow arrow).

Fluorescein angiography (FAG) of the left eye (A, B) early FAG had delayed perfusion of both veins and arteries. (C) and late phase vessel and disc leakage (arrows).
망막혈관염의 다른 원인을 감별하고자 혈액검사를 시행하였다. 일반 혈액검사, 적혈구침강속도, C-반응단백질은 모두 정상이었고, 간기능, 혈중요소 질소, 크레아티닌, 전해질 수치, 소변 수치 모두 정상이었다. 혈액응고검사에서 prothrombin time, international normalized ratio, activated par tial thromboplastin time은 정상 범위 내에 있었다. 혈청학적 검사에서 간염표지자, 항핵항체, venereal disease research laboratory, antineutrophil cytoplasmic antibody 등은 음성이었다. 치료를 시작한 지 1주일 후, 좌안의 충혈과 통증은 호전되었다. 좌안 최대교정시력은 안전수지 30 cm로 측정되었으며, 세극등현미경검사상 각막후면침착물 및 전방세포 및 유리체세포 호전이 관찰되었다. 안저검사 결과 유리체 부유물은 계속되었고(Fig. 3B), 빛간섭단층촬영에서 망막하액은 감소하였다(Fig. 1C). 환자의 비문증을 해결하기 위해 좌안 유리체절제술을 계획하였고, 위수정체안으로 25게이지 평면부 유리체절제술(EVA®, Dutch Ophthalmic Research Center Inc., Zuidland, Netherlands)만을 시행하였으며, 유리체 검체는 채취하지 않았다.
수술 후 1주일이 지난 시점에서, 좌안의 최대교정시력은 여전히 안전수지 30 cm였고, 세극등현미경검사상 좌안 각막후면침착물 대부분이 감소하였다. 또한, 전방 및 유리체 세포는 관찰되지 않았으며, 유리체 부유물은 사라졌으며(Fig. 3C), 빛간섭단층촬영에서 망막하액은 감소하였다(Fig. 1D). 경구 스테로이드 치료는 중단되었으며, 좌안 프레드포르테 안약를 하루에 4번 점안하며 경과 관찰하기로 결정하였다. 수술 후 1달이 경과한 시점에서, 좌안 최대교정시력은 0.15로 호전되었고 안내 염증은 호전되었으나, 빛간섭단층촬영에서 망막하액이 있어 베바시주맙(Avastin®, Genetech, Inc.) 안내 주사를 시행하였다. 이후 망막하액 및 망막 내 낭포 소견이 지속되어 애플리버셉트로 교체하여 주사가 시행되었으며, 브롤루시주맙 연관 망막혈관염 발병 후 1년째 재발 없이, 좌안 최대교정이 0.5로 측정되었다.
고 찰
나이관련황반변성의 유병률은 증가하고 있으며, 이에 따른 사회경제적 부담도 증가하고 있다. 습성 나이관련황반변성의 표준 치료는 유리체강 내 항혈관내피성자인자 주사 치료이다. 최근 출시된 브롤루시주맙의 교체 투여를 통해 이전 항혈관내피성장인자 약제에 반응이 제한적인 경우에도 일부에서 뚜렷한 해부학적인 호전을 얻을 수 있는 것으로 보고되었다.4,6
브롤루시주맙 주사 후 합병증을 보면, HAWK와 HARRIER의 post hoc review3에 따르면 브롤루시주맙(1,088안 중 50 증례, 4.6%)은 애플리버셉트(729안 중 8증례, 1.1%)에 비해 더 높은 안내 염증 발생률을 보였다. 일본의 연구에서 단기간 안내 염증 발생률은 9.4%로 보고하였는데7, 이는 HAWK와 HARRIER post-hoc review보다 높았다. 또한, HAWK 연구에 참여한 일본 환자들의 안내 염증 발생률은 다른 인종의 환자보다 두 배에서 세 배 높았으며,8 이는 인종 간 차이가 원인일 수 있다. 이러한 높은 안내 염증의 발생률 때문에 브롤루시주맙 사용 시 주의가 필요하다. 항VEGF 약물의 유리체강 내 주사 후 비감염 안내 염증은 다른 약제들에서도 보고되었다.9 그러나 브롤루시주맙의 경우 혈관폐쇄망막병증까지 보고되었고, 염증으로 인한 지속적인 시력 저하 증례도 있었다.3,10,11
브롤루시주맙은 단클론 단일 사슬 단편 인간화항체로 분자량은 26 kDa으로, 이는 기존의 항혈관내피성장인자 약제보다 작다. 이 약제는 0.05 mL 부피당 6 mg이 함유되어 있어, 동일 부피의 애플리버셉트 2 mg보다는 12배, 라니비주맙 0.5 mg보다는 22배 농도로 분자가 포함되어 있다.12 브롤루시주맙의 작은 분자량은 조직 내에서의 용이한 침투와 빠른 약효 발현을 가능하게 하며, 높은 농도로 인해 약효를 더 오래 유지시킨다. 이로 인해 항혈관내피성장인자 효과가 뛰어나다고 할 수 있다.13 그러나 이러한 특성은 높은 안 내 염증 발생의 원인이 될 수 있다. Haug et al14에 따르면, 브롤루시주맙의 높은 유리체강 내 농도는 혈액망막장벽이 파괴된 나이관련황반변성 상태에서의 면역 체계로의 잦은 노출로 이어지며, 이로 인해 안내 염증의 위험이 증가할 수 있다고 제안하였다.
브롤루시주맙 주사 후 안내 염증의 치료에 대한 명확한 가이드라인은 아직 없으나, 전문가 의견을 요약한 연구 논문이 2020년에 발표된 바가 있다.15 본 연구에서는 브롤루시주맙 연관 안내염을 안내 염증만 있는 경우, 안내 염증 및 망막혈관염이 있는 경우, 안내 염증 및 망막혈관염 그리고 혈관폐쇄망막병증이 동반된 경우 세 가지로 분류하였다. 그리고 브롤루시주맙 연관 안내염이 확진된 경우 경구 스테로이드, 스테로이드 점안제, 스테로이드 테논낭하 주사, 유리체강 내 스테로이드 약물 주입술 등을 포함한 적극적인 염증 치료를 시행하고, 특히 혈관폐쇄망막병증이 동반된 경우는 유리체절제술을 고려할 것도 제안하고 있다.
경구 및 국소 스테로이드 치료로 호전된 증례들을 살펴보면, 국내의 경우,5 이전 베바시주맙 및 애플리버셉트 치료를 받았던 적이 있으며 브롤루시주맙 교체 투여 후 8주 시점에 결막 충혈, 시력저하, 안압상승과 함께 안내 염증 반응 및 망막 허혈 소견이 발견되어 브롤루시주맙 치료 관련 안내 염증으로 진단하였다. 경구 및 점안 스테로이드 투여 및 트리암시놀론 테논낭하주사로 증상 호전을 보였다. Kataoka et al10 또한 경구 스테로이드 및 점안 스테로이드 투여, 트리암시놀론 테논낭하 주사로 증상 및 시력이 호전된 브롤루시주맙 연관 망막혈관염 3개의 증례를 보고하였다. 세 개의 증례 중 두 증례는 이전 안내 주사를 투여 병력이 없었으며, 한 증례는 애플리버셉트에서 브롤루시주맙으로 교체 투여 후 발생한 증례였다.
반면 스테로이드 치료에도 시력 호전이 없는 증례도 있다. Barchichat et al11은 양안 브롤루시주맙 주사 후 양안 망막혈관염이 발생한 사례를 보고하였는데, 이 환자 역시 이전에 다른 항-VEGF 약물을 받은 경력이 있었으며, 본 환자와는 달리 첫 번째가 아닌 두 번째 브롤루시주맙 주사 후 발생하였다. 이 환자의 경우 브롤루시주맙 관련 망막혈관염 진단 후 정맥 및 점안 스테로이드 치료, 트리암시놀론테논낭하 주사를 시행하였다. 망막혈관염의 호전은 있었으나 시력 호전은 없었다.
우리 증례의 환자는 이전 수차례 라니비주맙 및 애플리버셉트를 투여받았던 병력이 있었다. 초기 내원 시 시행한 혈액검사상 감염이나 면역 질환을 의심할 만한 소견은 발견되지 않았고, 브롤루시주맙 주사 1주 이후에 증상이 발생한 점에서 브롤루시주맙 연관 안내 염증을 의심하여 경구 및 점안 스테로이드, 트리암시놀론 테논낭하 주사를 시행하였다. 스테로이드 치료 후 증상 호전 및 각막후면침착물 및 전방 내 염증세포가 감소하였다. 2020년 전문가 의견을 요약한 연구 논문15에서 브롤루시주맙과 연관된 안내염의 치료 방향에 대한 논의가 있었다. 이 중 혈관폐쇄망막병증을 동반하지 않은 브롤루시주맙 연관 안내염의 경우 약물 치료를 권고하였다. 또한, Kataoka et al10은 혈관폐쇄망막병증을 동반하지 않은 브롤루시주맙 연관 안내염에서 유리체절제술 없이 국소 및 전신 스테로이드 치료만으로 시간이 지남에 따라 호전되는 증례를 보고하였다. 그러나 이전 증례10,15와 비교해 본 증례는 초기 최대교정시력이 더 낮았고, 치료 시작 1주 후 최대교정시력의 호전이 더디었기에, 유리체강 내 브롤루시주맙 농도 및 염증매개체의 농도를 줄이기 위해15 유리체절제술을 시행하였다. 이후 양호한 망막 해부학 및 시력 예후를 보여주고 있다.
브롤루시주맙 연관 안내 염증 반응이 확인되는 경우 국소 및 경구 스테로이드 치료, 유리체절제술 등 적극적인 치료를 하는 것이 중요하며, 적극적인 치료를 통해 양호한 망막 해부학 및 시력 결과를 얻을 수 있음을 본 증례를 통해 보고한다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
이다빈 / Dabin Lee
단국대학교병원 안과학교실
Department of Ophthalmology, Dankook University Hospital
