전형적인 교감안염 환자의 다양한 영상학적 검사: 증례 보고
Multimodal Imaging Assessment of Typical Sympathetic Ophthalmia: A Case Report
Article information
Abstract
목적
교감안염은 최근 낮은 발병률을 보이지만, 양안의 시력저하를 초래할 수 있어, 신속하게 진단을 내리는 것이 매우 중요하다. 저자들은 특징적인 여러 가지 영상학적 검사 결과와 함께 전형적인 교감안염의 환자 증례를 보고하고자 한다.
증례요약
양안 백내장수술과 우안 인공수정체 공막고정술의 과거력이 있는 64세 남자 환자가 3주 전 넘어지면서 심한 둔상을 입고 우안의 통증과 시력저하를 주소로 뒤늦게 내원하였다. 우안에 공막절개창을 통한 홍채의 탈출과 전방 출혈이 있어, 일차 봉합술을 시행하였다. 수술 1주 뒤, 환자는 반대안인 좌안의 시력저하를 호소하였고, 광각안저촬영, 빛간섭단층촬영, 형광안저혈관조영술에서 다발성 국소 과형광 누출과 장액성 망막박리가 확인되었다. 우안의 외상력과 좌안의 검사 결과를 통하여 저자들은 교감안염으로 진단하였고, 정맥을 통한 고용량 스테로이드 치료를 시행하자 환자의 증상은 호전되었다.
결론
본 증례의 환자는 교감안염의 특징인 여러 차례 안과적 수술 이력 및 반대안의 외상 이력이 있었고, 영상학적 검사 결과 또한 매우 전형적인 소견을 보인다. 본 증례보고를 통해 교감안염을 초기에 진단하고 치료하는 데 도움이 되었으면 한다.
Trans Abstract
Purpose
Despite the relatively low incidence of sympathetic ophthalmia, prompt diagnosis is essential to prevent visual impairment in both eyes. Here, we present a case of sympathetic ophthalmia, emphasizing distinctive imaging findings.
Case summary
A 64-year-old male patient presented with complaints of right ocular pain and visual disturbances occurring 3 weeks after blunt trauma. The patient had a history of ophthalmologic surgeries, including cataract surgery in both eyes and intraocular lens trans-scleral fixation in the right eye. A primary suture was performed in the right eye due to iris prolapse through the scleral incision site and anterior chamber hemorrhage. At 1 week post-surgery, the patient reported diminished visual acuity in the left eye. Further assessment using wide-field fundus photography, optical coherence tomography, and fluorescein angiography revealed multiple focal hyperfluorescence leakage and serous retinal detachment. Consequently, sympathetic ophthalmia was diagnosed. Intravenous administration of high-dose steroids led to significant symptom improvement.
Conclusions
We present a patient with a history of multiple ophthalmic surgeries and contralateral eye trauma indicative of sympathetic ophthalmia. Imaging modalities revealed typical findings for this condition. This case report emphasizes the importance of early diagnosis and treatment of sympathetic ophthalmia.
교감안염은 육아종성 범포도막염으로, 안구 내 수술 또는 안구의 천공성 외상 이후에 발생하는 매우 흔하지 않은 질환이다.1 기존의 보고에 따르면 발생 빈도는 선행 사건 후 0.044-0.190%로 알려져 있으며, 대부분의 경우는 1년 이내에 발생한다.2-4 교감안염이 특정 성별, 인종 또는 연령에서 유의하게 더 높은 발생 경향을 보이지는 않는다고 알려져 있으나 일부 연구에서는 남성에서 더 높은 비율로 발생한다는 연구가 있다. 하지만 이는 남성이 여성에 비해 안구의 천공성 외상을 당할 위험에 더 많이 노출되어 있기 때문이라고 추정하였다. 또 다른 연구에서는 전체 연령 중 어린이 또는 60세 이상의 노인 인구에서 더 높은 빈도로 발생한다고 보고되었는데, 이는 젊은 연령에서 안구 외상 위험이 높을 가능성과 노인 인구에서 안구수술 빈도가 증가하는 요인이 반영된 것으로 여겨진다.1 교감안염의 치료를 위해서는 고용량의 스테로이드제가 필요하며 때로는 면역억제제가 필요할 수 있다.2,3 따라서 치료가 잘못 이루어지거나 약제에 반응이 없을 경우 양안의 시력상실이 유발될 수 있기 때문에 교감안염의 정확한 진단 및 치료는 중요하다.
저자들은 반대안에 여러 차례 수술 과거력이 있으면서, 3주 전 심한 둔상을 받고 안과적 수술을 받은 1주일 후 발생한 전형적인 교감안염 환자를 접하였기에, 본 증례를 통하여 교감안염의 진단에 중요한 특징적인 영상학적 검사 결과들을 보고하고자 한다.
증례보고
64세 남자 환자가 우안 시력저하를 주소로 내원하였다. 환자는 내원 3주 전 넘어지면서 우안을 수상당하였지만 안과적 진료 및 치료 없이 지내던 중, 진행하는 우안의 통증, 눈꺼풀부종, 결막충혈 그리고 시력저하로 내원하였다. 전신 질환으로 고혈압과 당뇨가 있었으며, 안과적으로 10년전 우안 백내장수술, 2년 전 좌안 백내장수술 그리고 1년 전 우안의 인공수정체 탈구로 인한 유리체절제술 및 인공수정체 공막고정수술을 받은 과거력이 있었다. 세극등현미경검사 결과, 과거 우안 수술 당시 절개창 부위가 벌어져 있었고, 홍채가 상처에 끼어 있었다(Fig. 1A, B). 스넬렌시력은 우안 광각 유, 좌안 0.9로 측정되었고, 우안 안압 14 mmHg, 좌안 안압 16 mmHg로 측정되었으며, 좌안은 전안부에 특이사항 없었고 안저검사에서 망막전막 외에 다른 이상 소견은 없었다(Fig. 1C, D). 이에, 우안 공막봉합술 및 전방세척술을 시행하였으며 수술 후 moxifloxacin hydrochloride (Moroxacin®, Hanmi, Seoul, Korea) 점안약과 ofloxacin (Tarivid®, Santen Pharmaceutical Co., Ltd., Osaka, Japan) 연고를 점안하였고 스테로이드 제제는 사용하지 않았다.
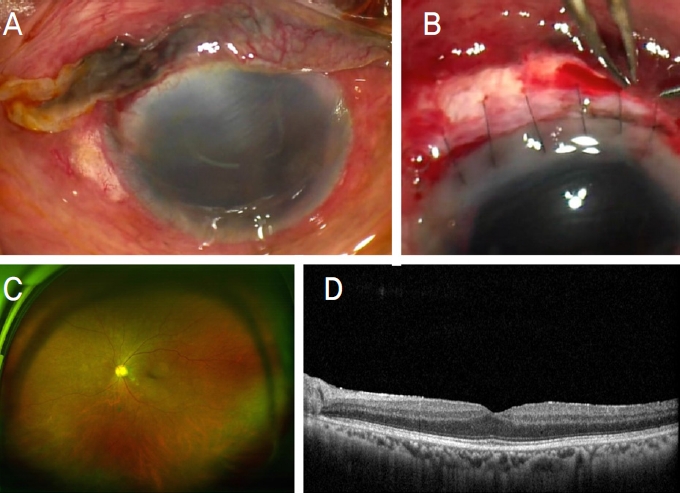
A 64-year-old male, right eye injured 3 weeks ago. (A) Preoperative findings of the right eye: conjunctival hyperemia, hyphema, and prolapsed iris. (B) Intraoperative findings of the right eye: the previous corneal wound was opened due to trauma and primary repair was done. (C, D) Initial findings of the left eye on wide fundus photography and optical coherence tomography: Snellen visual acuity of the left eye was 0.8 and faint epiretinal membrane is observed.
수술 1주 뒤, 환자는 진행하는 좌안의 시력저하를 호소하였다. 스넬렌 시력 우안 광각 유, 좌안 0.3, 좌안 전방세포 1+ 관찰되었으며, 유리체혼탁 및 유리체 내 염증 소견이 관찰되었고 빛간섭단층촬영에서 소량의 망막하액이 확인되었다(Fig. 2A-D). 당시 임상의는 이를 특발성 포도막염으로 진단하였고, 1% prednisolone acetate (Predforte®, Allergan Korea, Seoul, Korea) 점안약 및 prednisolone (Solondo®, Yuhan, Seoul, Korea) 50 mg 경구 스테로이드 투여로 치료를 하였고, 경구 스테로이드는 4일마다 10 mg씩 빠르게 줄였다. 약물 치료 초기에는 스넬렌시력 우안 광각 유, 좌안 0.7, 좌안 전방세포 trace로 감소되면서 호전되는 양상을 보였으나 스테로이드를 감량하면서 사용한 지 약 20일 뒤 시력저하가 다시 발생하였다. 당시 검사에서 좌안에 전방 세포는 1+로 다시 증가하였고, 스넬렌시력표상 좌안 0.06으로 크게 감소하였다(Fig. 3A). 유리체혼탁 및 유리체 내 염증 소견을 보였고, 빛간섭단층촬영에서 소포성의 망막하액과 망막내액, 망막색소상피와 망막 사이의 띠, 맥락막주름 소견이 관찰되었다(Fig. 3C). 광각안저촬영과 형광안저혈관 조영술에서 다발성 국소 과형광 누출 및 이 부분으로 장액성 망막박리가 확인되었다(Fig. 3B, D, E). 이에 망막 분과로 환자가 의뢰되었고, 반대안의 외상력과 수술력, 상기 검사 소견을 통하여 좌안을 교감안염으로 진단하였다. 치료를 위해서 정맥을 통하여 methylprednisolone (Methysol®, Reyon, Seoul, Korea) 1,000 mg/day 스테로이드를 5일간 투여 후 경구 스테로이드로 변경하였고 60 mg으로 시작하여 1주일 간격으로 10 mg씩 차츰 감량하였다(Fig. 4A, B). 정맥을 통한 고용량 스테로이드 치료 후 스넬렌시력표로 측정한 좌안 시력 0.5, 전방세포 trace, 유리체혼탁 및 염증 소견 감소 양상을 보였으며, 안저에서 관찰되던 맥락막주름, 망막하액과 망막내액 감소 양상이 관찰되었다. 경구 스테로이드 치료까지 시행한 후에는 스넬렌시력표로 측정한 좌안 시력 0.9, 전방 세포는 관찰되지 않았고 망막맥락막 병변과 환자의 증상은 호전되었으며 재발 없이 유지되었다.
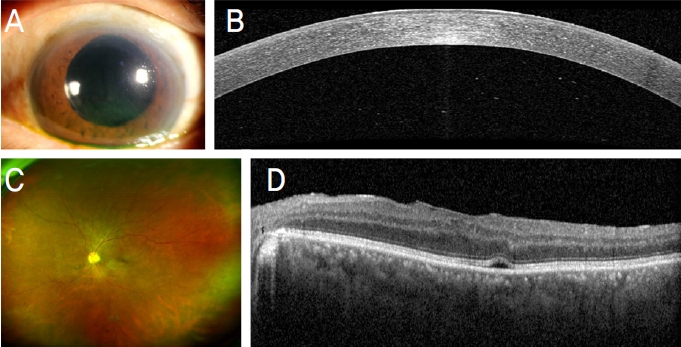
Anterior segment and fundus examination of the left eye one week after the right eye surgery. (A, B) In the left eye, anterior chamber cells were observed at a grade of 1+. (C, D) Vitreous opacities and vitreous inflammation were observed and a small amount of subretinal fluid was detected.
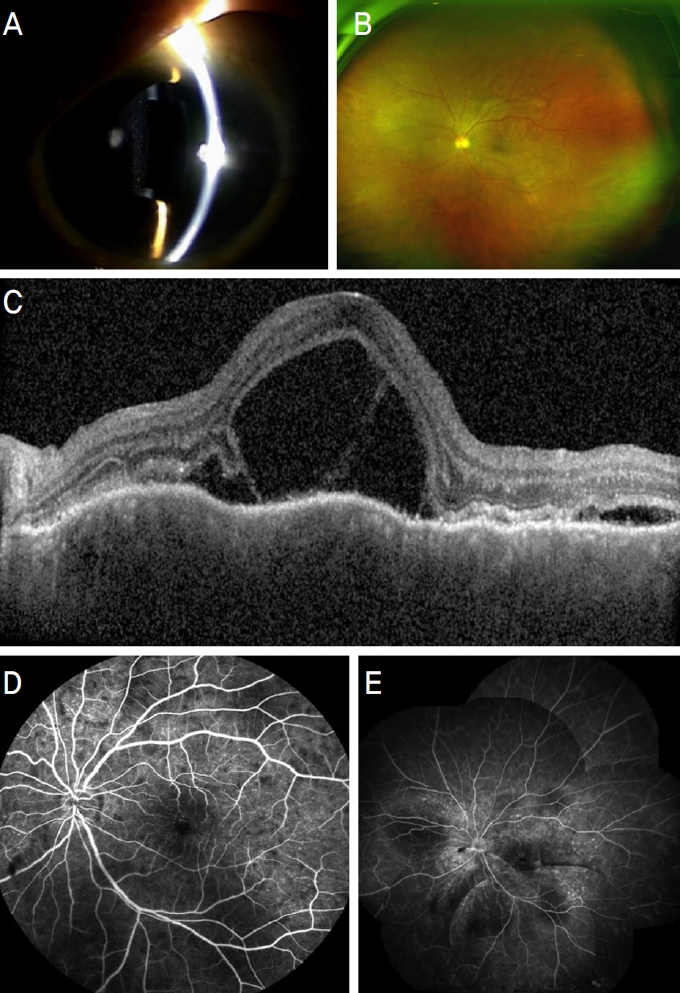
Anterior segment fundus examination of the left eye after discontinuation of 1% prednisolone acetate and oral prednisolone treatment. (A) Anterior segment photography. (B) Wide-angle fundus photography: there were multi-focal choroiditis with associated exudative retinal detachments. (C) Optical coherence tomography: loculated spaces of subretinal and intraretinal fluid with bands extending from the inner retina to the retinal pigment epithelium and choroidal folding was shown. (D) Early phase of fluorescein angiography. (E) Late phase of fluorescein angiography: multiple hyperfluorescent points of leakage with late pooling of dye in the areas of serous detachment were shown.
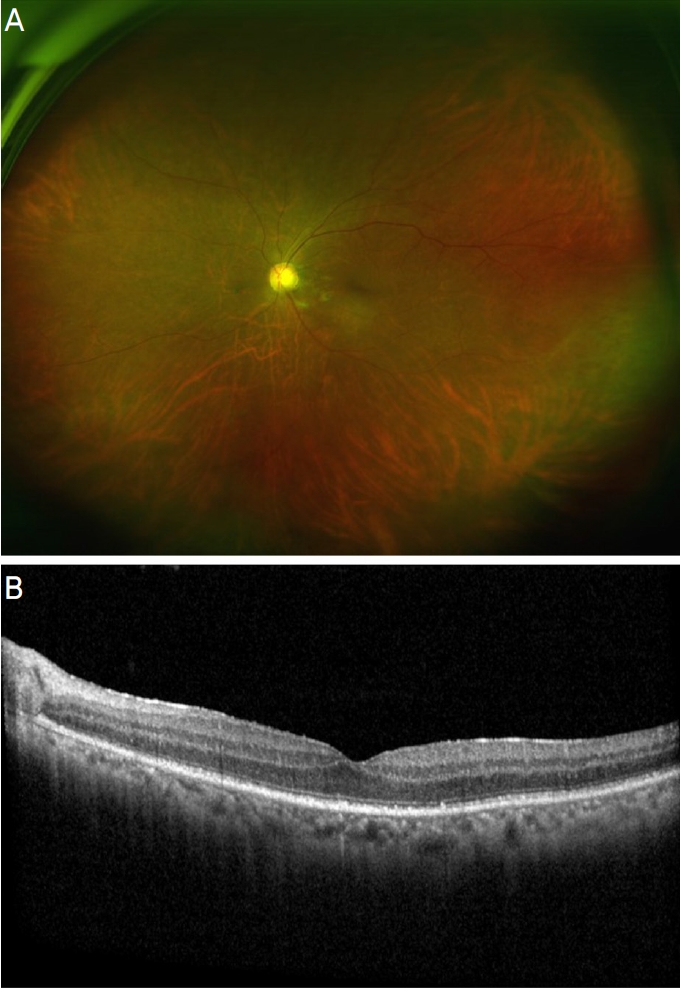
Wide-angle fundus photography (A) and optical coherence tomography (B) after 5 days of high-dose steroid treatment (intravenous, 1,000 mg/day).
고 찰
교감안염은 안구의 천공성 외상 또는 안 내 수술 후 수일에서 수개월 후 발생하는 흔치 않지만 치명적인 질환으로, 양안성 육아종성 포도막염이 특징적인 소견이다. 외상에 의해 발생하는 빈도는 전체 교감안염의 60-70%에 해당하며, 약 30%가 안구 내 수술에 의해 발생한다고 알려져 있다. 교감안염의 정확한 병태생리학적 기전은 밝혀지지 않았으나 유전적 요인이 관여한다고 알려져 있으며 human leukocyte antigen (HLA)-DRB1*4와 HLA-DQB1*04의 상호작용에 의한 T세포 매개 지연형 과민반응이 주요 기전으로 알려져 있다.5-7 경한 통증, 눈부심, 눈물흘림, 시력저하 등의 증상을 보일 수 있으며, 삼출성 망막박리 및 시신경부종, 맥락막 탈색 소견과 망막색소상피의 변화를 보일 수 있다.8,9 본 증례의 환자에서 안구 내 염증이 발생하였고 형광안저혈관조영술 및 빛간섭단층촬영에서 망막하 공간 형광 고임을 보이며 삼출성 망막박리가 관찰된 것은 보크트-고야나기-하라다병과 유사한 점이다.10 그러나 환자의 경우 안구에 천공성 손상을 입은 과거력이 있고 경과 관찰 동안 보크트-고야나기-하라다병에서 특징적으로 관찰될 수 있는 신경학적 증상, 청각이상 및 탈색소 병변과 같은 안구 외적인 증상이 보이지 않았다는 점을 바탕으로 교감안염을 진단할 수 있었다.11,12
교감안염의 치료 방법으로는 고용량의 경구용 스테로이드를 최소 6개월 동안 유지한 후 점차적으로 줄여 나가는 것이 주된 치료 방법으로 알려져 있다. 그러나 스테로이드를 장기간 사용할 수 없거나 치료 효과가 부족할 경우 T세포가 매개하는 지연형 과민반응을 조절하기 위한 방법으로 azathioprine, cyclosporine, methotrexate와 같은 면역억제제를 사용할 수 있다.2,3 교감안염의 치료로 고용량 스테로이드를 사용하기 앞서, 중심성 장액성 맥락망막병증과의 감별이 중요한데 이는 교감안염과 달리 중심성 장액성 맥락망막병증의 경우 스테로이드 사용이 증상을 악화시킬 수 있기 때문이다. 본 증례 환자의 경우 빛간섭단층촬영에서 망막하액에 의한 삼출성망막박리가 관찰되는 점은 중심성 장액성 맥락망막병증과 유사하지만 망막하액과 망막외층의 낭포 형성이 관찰되는 점에서 차이가 있으며, 형광안저혈관조영술에서 잉크얼룩(ink-blots) 또는 굴뚝연기(smoke-stacks)와 같은 모양이 아닌 다발성 국소 과형광 누출이 보이는 점에서 중심성 장액성 맥락망막병증을 감별할 수 있었다(Fig. 3C-E).13 또한 치료를 위하여 고용량의 스테로이드를 사용하자 증상이 완전히 호전되었다(Fig. 4A, B).
본 증례의 환자는 여러 차례의 안과적 수술을 받은 과거력, 반대안의 심한 외상력, 교감안염에서 보일 수 있는 영상학적 검사 결과를 보였다는 점에서 매우 전형적인 교감 안염 환자로 생각된다. 교감안염의 빠른 진단은 양안의 시력저하를 막을 수 있기에, 환자의 시력 예후뿐만 아니라 삶의 질을 보존하는 것에 큰 도움이 될 것이다. 저자들은 전형적인 교감안염을 보이는 본 증례의 환자를 보고 함으로써, 이를 통하여 임상의들이 근래 발병률이 낮아 간과하기 쉬운 교감안염을 진단하는 데 도움이 되었으면 한다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
박세익 / Se Ik Park
창원경상국립대학교병원 안과
Department of Ophthalmology, Gyeongsang National University Changwon Hospital
