망막분지정맥폐쇄 환자의 주사 치료 후 시력 및 중심황반두께와 맥락막혈관지수 관련성 분석
Choroidal Vascularity Index and Treatment Outcomes in Branch Retinal Vein Occlusion Patients with Macular Edema
Article information
Abstract
목적
황반부종을 동반한 망막분지정맥폐쇄 환자의 유리체 내 주사 치료 이후 황반부종의 감소 및 시력 개선 정도와 맥락막혈관지수의 관련성을 알아보고자 한다.
대상과 방법
2017년 1월부터 2020년 10월까지 망막분지정맥폐쇄를 진단받고 유리체 내 항혈관내피성장인자 주사 치료(27안) 혹은 덱사메타손 이식제 치료(23안)를 한 환자들을 대상으로 후향 분석하였다. 빛간섭단층촬영을 이용해 해당안과 반대안의 중심황반두께, 황반하 맥락막두께 및 맥락막혈관지수를 측정하여 주사 치료 이후 6개월째 중심황반두께 및 시력 호전 정도와의 상관성을 분석하였다.
결과
주사 치료 후 6개월째 시력과 중심황반두께가 호전되었다. 다중선형회귀분석상 6개월 후 시력 개선 정도와 관련 있는 인자는 반대안 맥락막혈관지수(표준베타계수=0.346, p=0.008), 빛수용체 타원체구역 온전성 정도(표준베타계수=0.398, p=0.001) 및 초기 시력(표준베타계수=0.590, p<0.001)이었다. 6개월 후 중심황반두께 감소 정도와 관련 있는 인자는 초기 중심황반두께였다(표준베타계수=0.563, p<0.001).
결론
황반부종이 심한 경우 빛간섭단층촬영에서 신호 가려짐으로 인해 정확한 맥락막혈관에 대한 평가가 어려울 수 있다. 본 연구에서는 반대안의 맥락막혈관지수가 클수록 황반부종을 동반한 망막분지정맥폐쇄 환자에서 치료 후 시력 개선 정도가 큰 것으로 나타났다. 맥락막혈관지수는 망막분지정맥폐쇄의 치료 예후를 예측하는 데 도움이 될 수 있으며, 이는 맥락막혈관 상태가 망막분지정맥폐쇄의 병태생리에 관여할 수 있음을 시사한다.
Trans Abstract
Purpose
To explore the association between the visual and anatomical outcomes and the choroidal vascularity index (CVI) post-intravitreal injection in patients with macular edema associated with branch retinal vein occlusion (BRVO).
Methods
We conducted a retrospective review of medical records of 50 patients (27 eyes treated with anti-vascular endothelial growth factor and 23 eyes treated with a dexamethasone implant) with BRVO and macular edema who underwent intravitreal injections from January 2017 to October 2020. We measured the central macular thickness (CMT), subfoveal choroidal thickness, and CVI of the BRVO eyes and the fellow eyes using optical coherence tomography and then analyzed the correlation between these measurements and visual and anatomical outcomes.
Results
After six months of treatment, the best corrected visual acuity improved, and CMT decreased. Multiple linear regression analysis revealed that factors associated with best corrected visual acuity improvement at six months were fellow eye CVI (standardized β = 0.346, p = 0.008), ellipsoid zone integrity (standardized β = 0.398, p = 0.001), and initial best corrected visual acuity (standardized β = 0.590, p < 0.001). Initial CMT (standardized β = 0.563, p < 0.001) was the only factor associated with the decrease in CMT at six months.
Conclusions
In cases of severe macular edema, accurate evaluation of choroidal vessels can be challenging due to shadowing. We discovered that a larger CVI in the fellow eye was associated with greater visual improvement in patients with BRVO and macular edema. CVI could be a prognostic factor for predicting treatment outcomes in BRVO patients, suggesting that the choroidal vascular status may play a role in the pathophysiology of BRVO.
망막분지정맥폐쇄는 시력 상실을 야기하는 망막혈관 질환 중 당뇨망막병증에 이어 두 번째로 흔한 질환으로 유병률은 0.3에서 0.9%로 보고되고 있다.1-4 망막분지정맥폐쇄로 인한 시력 상실의 주요 기전은 황반부종이다. 황반부종은 모세혈관내피세포의 밀착연접의 손상으로 인한 혈액망막장벽의 파괴, 혈관내피성장인자나 인터루킨-6 등의 혈관 투과성을 변화시키는 염증성 인자들로 인해 혈관 내에서 주변 조직으로 체액의 이동이 유발되어 발생한다.5-7
최근 이미징 기술의 발달로 빛간섭단층촬영 깊이증강모드(enhanced depth imaging)를 이용해 맥락막의 정량적 관찰이 가능해졌다. 이러한 기술을 통해 망막분지정맥폐쇄의 병태생리에는 망막뿐 아니라 맥락막도 연관되어 있다는 연구 결과들이 보고되었다.8 또한 단순한 맥락막의 두께 측정 뿐 아니라 맥락막혈관지수(choroidal vascularity index, CVI)라는 새로운 변수를 도입하여 빛간섭단층촬영에서 얻은 맥락막 영역을 혈관 영역과 기질 영역으로 나누고 전체 맥락막 영역에서 혈관 영역이 차지하는 비율을 구하였다.9,10 맥락막혈관지수를 이용한 최근 연구 결과들을 살펴보면, 망막분지정맥폐쇄가 있는 환자의 병변안의 맥락막혈관지수가 질환이 없는 반대안의 맥락막혈관지수보다 낮았으며, 진단 당시의 병변안의 맥락막혈관지수는 치료 2년 뒤 안정된 상태의 병변안의 맥락막혈관지수보다 낮았다. 반대안의 맥락막혈관지수는 장기적인 시력 예후와 관련이 있었는데, 진단 당시 맥락막혈관지수의 값이 클수록 장기 시력 예후가 좋았다.11-14 이러한 연구 결과들을 종합해보면 망막분지정맥폐쇄의 병태생리에 맥락막혈관의 상태가 깊이 관여되어 있음을 알 수 있다.12,15
망막분지정맥폐쇄와 연관된 황반부종에 대해서는 유리체 내 항혈관내피성장인자 또는 덱사메타손 주사를 통해 치료를 하며, 빛간섭단층촬영을 통해 황반부종의 변화 추이를 추적 관찰한다.16,17 본 연구에서는 망막분지정맥폐쇄 환자의 병변안 및 반대안의 맥락막혈관지수를 통해 시력 및 중심황반두께 변화 등 황반부종 주사 치료의 치료 효과를 예측할 수 있는지 알아보고자 한다.
대상과 방법
2017년 1월부터 2020년 10월까지 본원 안과에 내원하여 단안의 망막분지정맥폐쇄로 진단받고 유리체 내 주사 치료 후 6개월 이상 추적 관찰하였던 환자 50명을 대상으로 후향적 분석을 진행하였다. 모든 과정은 헬싱키선언(Declaration of Helsinki)을 준수하였으며 강동성심병원 임상연구윤리심의위원회(Institutional Review Board; 승인번호 2023-01-001)의 승인 후 진행되었다.
본 연구의 포함 기준은 망막분지정맥폐쇄로 유리체 내 항혈관내피성장인자 혹은 덱사메타손 주사를 맞은 18세 이상 성인을 대상으로 하였으며, 제외 기준은 다음과 같다: 1) 황반변성, 당뇨망막병증, 녹내장 등 시력에 영향을 줄 수 있는 다른 안과 질환이 동반된 경우, 2) 6개월 이내 유리체 내 주사 치료를 받은 기왕력이 있는 경우, 3) 주사 치료 이후 6개월간 안저촬영 및 빛간섭단층촬영 추적검사를 시행하지 않았거나, 매체혼탁이 심해 이미지 분석이 어려운 경우.
환자들은 유리체 내 항혈관내피성장인자(ranibizumab; Lucentis®, Genentech Inc., South San Francisco, CA, USA/bevacizumab; Avastin®, Genentech Inc.) 혹은 덱사메타손(Ozurdex®, Allergan, Irvine, CA, USA) 주사를 맞았으며, 조사 기간 동안 주사 치료를 받은 환자 중 6개월 이내 주사 치료를 받지 않은 환자들만 모집을 하였고, 조사 기간의 첫 주사 시점을 기저 시점으로 설정하고 연구를 진행하였다. 총 50안 중 27안은 항혈관내피성장인자 주사 치료를 받았고, 23안은 덱사메타손 주사 치료를 받았다. 모든 환자는 내원 시 시력, 안압, 안저검사 그리고 빛간섭단층촬영검사(Spectralis OCT, Heidelberg Engineering Inc., Heidelberg, Germany)를 시행하였다.
중심황반두께는 중심부 1 mm 영역의 평균 황반두께로 정의하였으며 빛간섭단층촬영 프로그램에 내장된 소프트웨어를 이용하여 측정하였다. 맥락막혈관지수는 MATLAB 프로그램(MATLAB, MathWorks, Inc., Natick, MA, USA)을 통해 계산하였다. 각각의 빛간섭단층촬영 이미지의 중심와 정가운데 위치를 기기에 내장된 프로그램의 화살표 도구를 이용하여 수작업으로 노란색으로 표시해 이후 분석에서 자동으로 이미지의 중앙 부위를 인식할 수 있도록 하였다. 맥락막 영역의 위쪽 경계인 망막색소상피/브루크막 복합체의 고반사선은 MATLAB 코드를 통해 자동으로 추출하였으며, 맥락막/공막 경계 부위는 ImageJ (version 1.47, National Institute of Health, Bethesda, MD, USA)의 선 그리기 도구를 이용하여 수작업으로 표시하였다. 자동으로 추출된 망막색소상피/브루크막 복합체의 경계에 오류가 있을 경우에는 수작업으로 다시 수정을 하였다. 이렇게 맥락막 영역이 결정되면 그 넓이와 황반하 맥락막두께(subfoveal choroidal thickness)는 자동 계산되었다. 또한 맥락막 영역을 Niblack 임계값을 이용하여 이분화시키고, 크기가 20픽셀 미만인 입자는 제거하여 노이즈를 제거하였다.18 중심와를 중심으로 비측 및 이측 2,500 μm씩 총 5,000 μm 영역에서 분석을 진행하였으며 맥락막혈관지수는 전체 맥락막 영역에 대한 혈관 내강 영역(어두운 영역)의 비율로 계산하였다(Fig. 1).
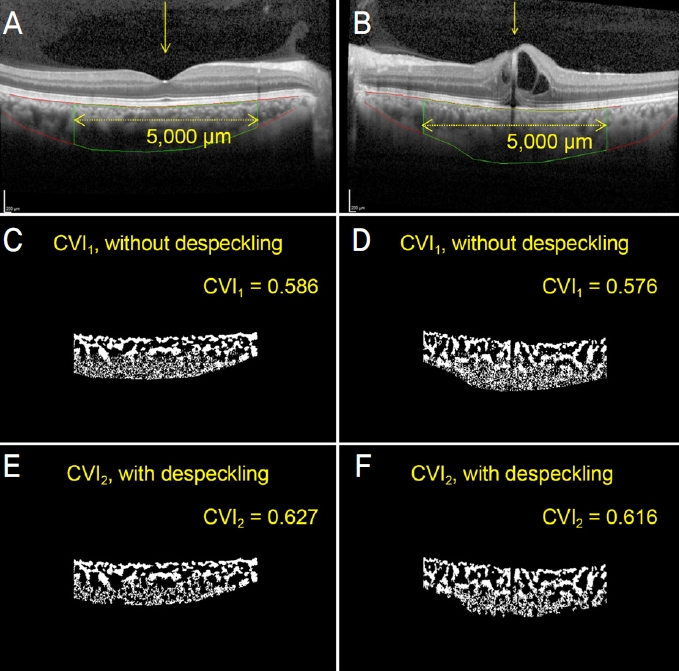
Choroidal vascularity index measurements. (A, B) The foveal center was marked with a yellow arrow using a built-in tool. The outer boundary of the choroid was manually drawn (lower red line). The lower border of the hyperreflective band of retinal pigment epithelium/Bruch’s membrane complex (upper red line) and the choroidal area of a predetermined range centered on the foveal center (green-bordered area) was automatically extracted. (C, D) Binarized images are obtained using the Niblack thresholding. (E, F) Images were despeckled with the removal of particles less than 20 pixels in size. The choroidal vascularity index (CVI) was calculated as the ratio of the luminal area (dark area) to the total choroidal area in the 5,000 μm range using both the original and despeckled binarized images.
황반부 두께 외에도 빛간섭단층촬영에서 관찰되는 빛수용체 타원체구역(ellipsoid zone)의 손상 정도를 0-2점으로 구분하여 비교하였다(2점: 황반부 빛수용체 타원체구역이 손상 없이 완벽히 연결되어 있음, 1점: 황반부 빛수용체 타원체구역이 일부 손상되어 완전히 연결되어 있지 않음, 0점: 황반부 빛수용체 타원체구역의 손상이 심해 관찰이 어려움). 또한 안저 사진에서 관찰되는 혈관이 매체혼탁에 의해 가려 보이는 정도를 이용하여 매체혼탁 정도를 정량적으로 분석하였다. 광각안저 사진(Optos, Optos PLC, Dunfermline, UK)에서 시신경유두를 기준으로 수직, 수평선을 그어 4개의 구역으로 나눈 뒤 각각의 구역에서 매체혼탁 정도를 0-2점으로 나누어 매겨(2점: 매체혼탁으로 인해 대부분의 주요 혈관궁[major vascular arcade]이 가려 보임, 1점: 매체혼탁으로 부분적으로 혈관궁이 가려 보임, 0점: 혈관궁이 명확히 관찰됨) 4분면의 점수를 합쳐 계산하였다(전체 0-8점) (Fig. 2).

Grading of the media opacity. Based on the optic disc, vertical and horizontal lines were drawn to divide the fundus photo into four quadrants, and the media opacity scores of each quadrant were summed (0-2 for each quadrant as score 0 for clearly visible vascular arcades; score 1 for partially obscured vascular arcades; score 2 for near completely obscured vascular arcades due to media opacity. 0-8 for the whole image). Examples of images and scores are shown in (A-C) where the total media opacity scores were 2, 5, and 8 respectively.
유리체 내 주사 치료 이후 6개월째 시력 호전 정도 및 중심황반두께 감소 정도와 관련된 인자들에 대해 다중선형회귀분석을 통해 분석하였다. 또한 반대안의 맥락막혈관지수 중앙값을 기준으로 두 군으로 나누어 두 군 간의 시력 및 중심황반두께 등 임상 양상을 비교하였다.
모든 통계적 분석은 SPSS for windows 27.0 버전(SPSS Inc., Chicago, IL, USA)을 이용하여 시행하였고 통계적인 유의수준은 p<0.05로 정하였다.
결 과
망막분지정맥폐쇄 환자 50명의 병변안과 반대안이 최종 분석에 이용되었으며, 환자의 평균 나이는 62.1 ± 10.1세, 남성의 비율은 38%였다. 27안(54%)은 항혈관내피성장인자 주사를, 23안(46%)은 덱사메타손 주사 치료를 받았다. 전체 환자 중 64% (32명)가 주사 치료 기왕력이 없는 첫 치료 환자였다. 항혈관내피성장인자 주사 치료군의 66.7% (18명), 덱사메타손 주사 치료군의 60.9% (14명)가 첫 치료 환자였으며, 첫 치료 환자의 비율은 두 치료군 사이에 통계적으로 유의미한 차이는 없었다(p=0.771). 기저 질환으로 58%가 고혈압이 있었으며, 22%가 당뇨병을 앓고 있었다. 42%는 인공수정체안이었다. 초기 시력은 logarithm of minimal angle resolution (logMAR) 0.50 ± 0.28이었으며 중심 5,000 μm 영역에서 측정한 맥락막혈관지수는 병변안 0.609 ± 0.033, 반대안 0.634 ± 0.032로 병변안의 맥락막혈관지수가 유의미하게 작았다(p<0.001) (Table 1).

Demographics and clinical characteristics of the study subjects
유리체 내 주사 치료 후 3개월 및 6개월째 시력과 중심황반두께 모두 통계적으로 유의하게 호전되었다. 초기 시력 logMAR 0.50 ± 0.28에서 3개월째 시력 logMAR 0.25 ± 0.27 (p<0.001), 6개월째 시력 logMAR 0.31 ± 0.30 (p=0.001)으로 호전된 결과를 보였으며, 중심황반두께도 초기 501.5 ± 154.2 μm에서, 3개월 394.3 ± 178.9 μm (p<0.001), 6개월 368.2 ± 150.7 μm (p<0.001)로 유의미하게 감소하였다(Table 1).
유리체 내 주사 치료 6개월 후 시력 호전과 관련된 인자로는 초기 시력(logMAR, standardized β=0.590, p<0.001), 빛간섭단층촬영에서 관찰되는 빛수용체 타원체구역 완전성 정도(standardized β=0.398, p=0.001) 및 반대안의 맥락막혈관지수(standardized β=0.346, p=0.008)가 있었다. 즉, 초기 시력이 나쁠수록 시력 호전 정도는 더 컸으며, 병변안의 타원체구역이 온전하거나 반대안의 맥락막혈관지수가 높은 것이 좋은 시력 예후와 관련이 있었다(Table 2). 주사 치료 6개월 후 중심황반두께의 감소 정도는 초기 중심황반두께와 관련이 있었으며, 초기 중심황반두께가 두꺼울수록 치료 6개월 후 두께 감소 폭이 컸다(standardized β=0.563, p<0.001) (Table 2).

Multiple linear regression analysis on visual gain and central macular thickness decrease 6 months after intravitreal injection treatment
반대안 맥락막혈관지수의 중앙값(0.631)을 기준으로 두 군으로 나누어 비교하였을 때 두 군 간의 나이, 성별, 기저 질환, 주사 치료제의 종류, 인공수정체 여부, 주사 치료 횟수, 초기 병변안의 맥락막혈관지수는 모두 통계적으로 유의미한 차이를 보이지 않았고, 주사 치료 이후 6개월째의 시력(logMAR)에서만 유의미한 차이를 보였다(반대안 맥락막혈관지수 낮은 군, 0.41 ± 0.35 vs. 반대안 맥락막혈관지수 높은 군, 0.20 ± 0.20; p=0.011) (Table 3).

Characteristics of two groups divided by fellow eye CVI
초기 반대안 맥락막혈관지수를 기준으로 나눈 두 군의 유리체 내 주사 치료 후 시력 및 중심황반두께의 변화를 보았을 때 중심황반두께는 비슷한 변화 양상을 보이지만, 시력의 경우 주사 치료 이후 2개월째부터 시력의 차이를 보이기 시작해 6개월째는 통계적으로 유의미한 차이를 보인다(Fig. 3). 두 군 간의 시력이 유의미하게 차이가 나는 6개월째 시점의 빛수용체 타원체구역의 손상 정도(반대안 맥락막혈관지수 낮은 군, 온전함 12안, 부분손상 8안, 손상 5안 vs. 반대안 맥락막혈관지수 높은 군, 온전함 11안, 부분 손상 11안, 손상 3안; p=0.941) 및 매체혼탁 정도(반대안 맥락막혈관지수 낮은 군, 2.0 ± 1.4 vs. 반대안 맥락막혈관지 수 높은 군, 1.8 ± 1.3; p=0.541)를 비교하였지만 두 군 간의 유의미한 차이는 발견할 수 없었다(Table 3).
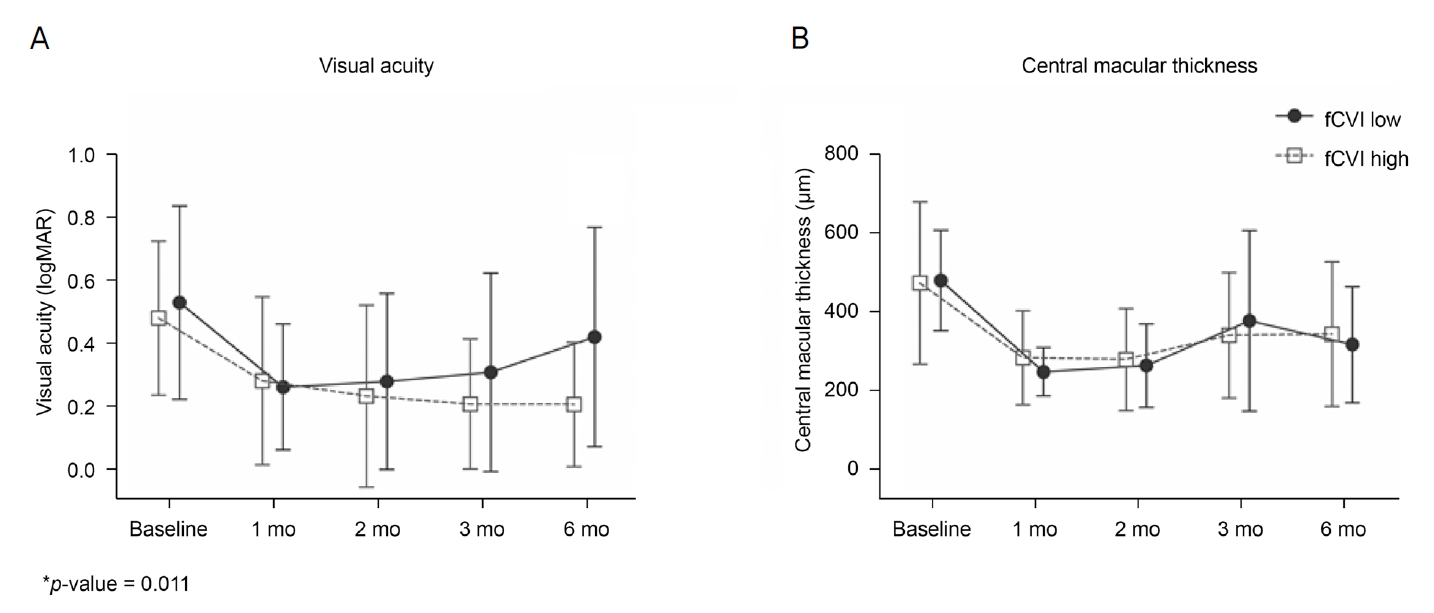
Comparison of best corrected visual activity and central macular thickness changes according to the fellow eye choroidal vascularity index. (A) Those with high fellow eye choroidal vascularity index showed better visual acuity at 6 months post-treatment. (B) No significant differences were observed between the two groups. fCVI = fellow eye choroidal vascularity index; mo = month(s). *p-value = 0.011.
고 찰
본 연구에서는 망막분지정맥폐쇄에 동반한 황반부종 치료 후 임상 경과에 맥락막혈관지수가 관련이 있는지 살펴 보았다. 치료 6개월째 중심황반두께 감소 정도는 초기 황반두께만 관련을 보여 맥락막혈관지수와의 유의미한 관련성은 찾을 수 없었다. 하지만 치료 6개월째 시력 개선 정도와 초기 반대안의 맥락막혈관지수가 관련성을 보여, 반대안의 맥락막혈관지수가 높을수록 시력 개선 정도가 큰 것으로 나타났다.
이전 망막분지정맥폐쇄에서 맥락막혈관지수에 대한 연구들에서 병변안의 맥락막혈관지수가 높을수록 치료 이후의 시력이 좋은 관련성을 보였다.11,19 Hwang et al11은 35명의 분지망막정맥폐쇄 환자를 대상으로 황반부종 당시의 병변안 및 반대안의 맥락막혈관지수와 2년 후의 시력 예후를 비교하였다. 해당 연구에서는 병변안의 맥락막혈관지수, 황반하 맥락막두께 및 반대안의 맥락막혈관지수가 2년 후의 시력과 유의한 상관성을 보였으며, 가장 관련이 높은 것은 반대안의 맥락막혈관지수였다. 이는 반대안의 맥락막혈관지수가 주사 치료 후 6개월째 시력 개선 정도와 관련성을 보인 본 연구와 유사한 결과이다. 다만 빛간섭단층촬영 이미지의 질에 영향을 미칠 수 있는 매체혼탁 정도나 시력에 영향을 미칠 수 있는 빛간섭단층촬영의 타원체영역의 온전성 등에 대한 평가 및 여러 인자의 효과를 고려한 다변량 분석은 시행되지 않았다.11
황반부종이 심한 경우 빛간섭단층촬영의 음영(shadowing)으로 인해 정확한 맥락막혈관에 대한 평가가 어려워 맥락막혈관지수의 측정 오류가 발생하기 쉽다. 본 연구에서도 병변안의 경우 맥락막의 경계를 찾는 것도 쉽지 않은 경우가 많았으며, 상측의 망막부종 부위의 고반사 영역에 의한 후방 음영으로 맥락막혈관 평가가 어려운 경우가 많았다. 실제 병변안의 맥락막혈관지수가 주사 치료 이후 임상 경과와 관련성을 보일 가능성은 있겠지만 본 연구에서는 유의미한 상관관계는 찾을 수 없었다. 대신 반대안의 맥락막 혈관지수를 분석에 포함하였을 때 주사 치료 후 시력 개선 정도와 유의미한 관련성을 보였다.
근시 소아를 대상으로 한 연구에 의하면 나이나 안축장 등은 맥락막혈관지수와 관련이 없었으나, 굴절률은 맥락막 혈관지수와 유의한 연관성을 보였다.20 양안의 맥락막두께 및 맥락막혈관지수의 대칭성을 살펴본 연구에 의하면, 맥락막두께는 정상인에서 양안 간에 높은 상관관계를 보였으며, 맥락막혈관지수는 양안 간에 중등도의 상관관계를 보였다. 특이하게도 우안이 좌안보다 맥락막두께가 더 두꺼웠고, 맥락막혈관지수는 더 작았다. 다만 그 차이는 임상적으로 유의미한 수준은 아니었다.21 이러한 기존 연구를 종합해 보면 양안의 굴절률에 큰 차이가 없고 특별한 안구 질환이 없다면 양안의 맥락막혈관지수도 대칭성을 보일 것으로 생각되며, 망막분지정맥폐쇄로 인한 병변안의 맥락막혈관지수의 변화, 황반부종으로 인한 측정 오차 등을 고려하였을 때 반대안의 맥락막혈관지수를 이용하여 병변안의 질병 이전의 맥락막혈관지수를 추정하는 것은 가능한 대안이 될 수 있을 것이다.
망막분지정맥폐쇄가 있는 눈에서는 맥락막혈관지수가 감소하며, 치료 이후에는 다시 증가하는 것으로 알려져 있다.11 우리 연구에서도 반대안의 맥락막혈관지수보다 병변안의 맥락막혈관지수가 더 작았다. 흥미롭게도 반대안의 맥락막혈관지수는 황반부종 치료 후 시력 예후와 관련성을 보였다. 맥락막혈관지수와 관련된 이전의 연구 결과들을 살펴보면, 맥락막혈관지수는 단순한 맥락막혈관의 상태뿐 아니라 관상동맥 질환과의 연관성도 보여 보다 전신적인 혈관 상태를 반영하는 지표로 생각된다.18 또한 혈액 투석을 받는 말기 신장병 환자에서 혈액 투석 이후 맥락막두께는 감소를 하였지만, 맥락막혈관지수는 유의미한 차이를 보이지 않아 맥락막혈관 상태를 보다 안정적으로 반영하는 지표로 생각된다.22 황반부종으로 인해 빛간섭단층촬영에서 정확한 맥락막 평가가 어려운 병변안 대신 맥락막을 보다 정확히 관측할 수 있는 반대안의 정보를 이용하는 것이 환자의 전반적인 기저의 맥락막혈관 상태를 평가하고 예측하는 데 더 타당할 것으로 생각된다. 실제 이전의 망막정맥폐쇄에서 주사 치료 이후의 시력 예후와 맥락막혈관지수의 상관성을 살펴본 연구에서도 병변안의 맥락막혈관지수보다 반대안의 혈관지수가 시력 예후와 조금 더 높은 연관성을 보였다.11
이러한 맥락막혈관지수와 시력 예후의 관련성은 맥락막혈관지수와 맥락막모세혈관 혈류와의 연관성으로 설명할 수 있겠다. 맥락막혈관지수가 높을 경우 맥락막모세혈관층의 혈류가 상대적으로 좋아 망막 허혈의 위험성을 낮추고, 체액 및 노폐물의 제거를 용이하게 하여 황반부종의 가능성을 낮추는 것으로 생각된다. Borrelli et al19에 따르면 황반부종이 동반된 망막분지정맥폐쇄에서 세포외액의 이동으로 인해 혈관 내강 영역이 감소하고 기질 영역이 증가하는 상황에서 혈관 내강 영역이 클수록 맥락막모세혈관 내 혈류가 더 큰 것으로 나타났다. 즉, 맥락막 혈류가 풍부한 맥락막혈관지수가 높은 환자의 경우 망막색소상피세포로의 산소 및 영양분 공급이 원활해지고, 망막내액 및 노폐물을 제거하는 작용이 수월해져 황반부종을 감소시키는 것으로 생각된다.
한편, 우리 연구에서는 반대안의 맥락막혈관지수에 따라 나눈 두 군 간에 중심황반두께의 차이는 없었다. 또 시력에 영향을 줄 만한 구조적인 원인인 매체혼탁이나 빛간섭단층촬영에서 관찰된 타원체구역의 온전성 등을 비교하였지만 시력 차이를 설명할 만한 소견은 관찰되지 않았다. 환자 수가 적어 유의미한 차이를 보이지 못했을 수 있으며, 아직 이미지에서 감별하기 어려운 초기 미세한 변화에 의한 차이의 가능성이 있겠다. 하지만 맥락막혈관지수가 좋은 군에서 황반부종 감소 외 다른 기전에 의해 시기능 회복을 도울 가능성도 고려해 봐야겠으며, 추후 추가적인 연구가 필요하겠다.
본 연구는 적은 환자 수, 짧은 추적 관찰 기간, 후향적 분석 방법 등 여러 제한점을 가지고 있다. 특히 반대안의 맥락막혈관지수가 망막분지정맥폐쇄에 동반한 황반부종 치료 후 시력 예후와 관련이 있음을 보였지만, 중심황반두께, 빛간섭단층촬영에서 보이는 타원체구역의 온전성 등 그 기전을 설명할 만한 구조적 차이를 밝히지 못한 점이 제한점으로 생각된다. 아직 영상 촬영에서 관찰되기 이전의 초기 미세한 차이가 있는지 살펴보기 위해 추후 더 많은 환자를 대상으로 장기간의 추적 관찰이 필요하겠다.
본 연구에서는 맥락막혈관지수가 망막분지정맥폐쇄 환자의 시력 예후와 관련성이 있는지 살펴보았다. 반대안의 맥락막혈관지수는 초기 시력이나 빛간섭단층촬영에서 관찰되는 타원체구역의 온전성과 독립적으로 황반부종 치료 6개월 후 시력 개선 정도와 연관성을 보였다. 맥락막의 혈류가 망막정맥폐쇄 및 황반부종의 회복에 관여하는 역할을 규명하기 위한 추가적인 연구가 필요하겠다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
Acknowledgements
This study was supported by the Korean Association of Retinal Degeneration.
References
Biography
최주원 / Ju Won Choi
한림대학교 의과대학 강동성심병원 안과
Department of Ophthalmology, Kangdong Sacred Heart Hospital, Hallym University College of Medicine
