맥락막비후가 있는 녹내장 안에서 아메드밸브삽입술 후 발생한 황반부 장액망막박리 증례
A Case of Macular Serous Retinal Detachment after Ahmed Valve Implantation in an Eye with Pachychoroid
Article information
Abstract
목적
맥락막비후가 있는 환자에서 아메드밸브삽입술 후 발생한 저안압과 관련된 황반부 장액망막박리를 보고하고자 한다.
증례요약
77세 남자 환자가 좌안의 조절되지 않는 안압을 주소로 방문하였다. 좌안 안압은 최대약물치료에도 불구하고 32 mmHg였고, 전방을 가득 채운 유리체가 발견되었다. 파장가변 빛간섭단층촬영검사에서 맥락막두께는 약 510 μm로 측정되어 맥락막비후가 관찰되었다. 전방 내 유리체를 제거하기 위해 유리체절제술을 시행하였고, 술 후 3주에 안압은 32 mmHg였다. 좌안에 아메드밸브삽입술을 시행하였고, 술 후 10일째 저안압이 발생하였다. 맥락막박리와 함께 빛간섭단층촬영검사에서 황반부 장액망막박리가 관찰되었다. 중심소와 아래 맥락막두께는 빛간섭단층촬영검사의 측정 범위를 넘어서 증가되었다. 저안압 교정을 위해 술 후 18일째 튜브 부분 결찰술을 시행하였다. 술 후 6주에 안압은 14 mmHg로 상승하였고, 장액망막박리는 사라졌고, 맥락막두께는 술 전 수치로 감소하였다.
결론
맥락막비후가 있는 환자에게서 아메드밸브삽입술 후 저안압이 발생하면 맥락막비후가 악화되며, 황반부 장액망막박리의 형태로 저안압 황반병증이 발생할 수 있다.
Trans Abstract
Purpose
We report a case of macular, serous retinal detachment associated with hypotony in a patient with pachychoroid disease developing after Ahmed valve implantation.
Case summary
A 77-year-old male visited our clinic with uncontrolled intraocular pressure (IOP; 32 mmHg) in his left eye despite maximal tolerable medical therapy. A prolapsed vitreous filled the anterior chamber. Swept-source optical coherence tomography (SS-OCT) revealed that the subfoveal choroidal thickness was about 510 μm, indicating pachychoroid. Vitrectomy was performed to remove the prolapsed vitreous. The IOP remained 32 mmHg 3 weeks after vitrectomy. Ahmed valve implantation was performed and hypotony developed 10 days postoperatively. Choroidal detachment was apparent and SS-OCT revealed macular accumulation of subretinal fluid. The subfoveal choroidal thickness increased to a level beyond the SS-OCT measurement range. Partial tube ligation was performed to treat the hypotony 18 days after Ahmed valve implantation; the IOP decreased to 14 mmHg at 6 weeks postoperatively. The macular, serous retinal detachment disappeared and the subfoveal choroidal thickness fell to the preoperative value.
Conclusions
Hypotony after Ahmed valve implantation can manifest as serous retinal detachment under the fovea accompanied by an increase in choroidal thickness in an eye with underlying pachychoroid.
파장가변 빛간섭단층촬영(swept-source optical coherence tomography, SS-OCT) 장비의 등장으로 망막하 맥락막의 구조를 관찰할 수 있게 됨에 따라 맥락막비후(pachychoroid)라는 개념이 사용되고 있다. 맥락막비후의 정의는 아직 확실히 확립된 바가 없으며 보고들마다 조금씩 정의를 달리하고 있는데, 일반적으로 파장가변 빛간섭단층촬영검사에서 중심소와 아래 맥락막두께가 300 µm를 넘는 경우를 의미한다.1 맥락막비후의 개념은 일반적으로 맥락막의 구조적인 변화와 기능적인 변화를 함께 통칭한다.2 맥락막비후를 가진 눈에서는 맥락막혈관의 직경이 커지고 투과성이 증대되고, 모세혈관이나 자틀러층(Sattler's layer)이 압축이 되어 두께가 얇아지기도 하는데, 보고들마다 이런 특징을 맥락막비후의 정의에 포함시키는 경우도 있고, 그렇지 않은 경우도 있다.3 맥락막비후가 맥락막색소상피의 변화를 동반하며 망막에 문제를 일으키는 경우는 맥락막비후 질환군(pachychoroid spectrum disease)이라고 하는데, 중심장액맥락망막병증이나 결절성맥락막혈관병증, 맥락막비후 색소상피병(pachychoroid pigment epitheliopathy), 시신경유두주위 맥락막비후 등을 모두 포함하는 포괄적인 질환군이다.4 맥락막비후 질환군에서 할러층 맥락막혈관의 직경이 커지면 상대적으로 맥락막의 압력이 높아지고 이차적으로 망막색소상피의 기능저하를 일으킬 수 있다고 생각되고 있다.4
저안압은 흔히 6.5 mmHg보다 낮은 안압을 뜻하고, 일반적으로 녹내장수술 후 3개월 이내에 안압이 5 mmHg 이하로 측정될 때로 정의한다.5 녹내장수술 후 발생하는 저안압 황반병증은 일반적으로 황반부 낭포황반부종과 관련된 황반부 두께 증가의 형태로 나타난다. 안압이 저하되어 망막 내 기질의 압력이 떨어지면 모세혈관의 압력이 세포 간 공간의 압력보다 높아져서 망막 모세혈관의 투과성이 증가하여 세포 사이 공간에 조직액이 축적되는 것이 그 기전 중 하나로 생각된다.6 또한 병태생리학적으로 저안압 상태에서는 공막이 안구 내측으로 찌그러지면서 포도막과 망막의 조직이 상대적으로 남게 되어 포도막과 망막에 주름이 생긴다고 보고 있다.7
저안압 황반병증이 빛간섭단층촬영검사에서 장액망막박리의 형태를 보이는 경우는 매우 드물고, 현재까지 보고된 문헌은 Kokame et al,8 Shimokawa et al,9 Park and Park10의 보고뿐이다. 또한, 아메드밸브삽입술 후 발생한 저안압 황반병증에서 황반하 장액망막박리를 보고한 문헌은 없었다.
저자들은 기존에 맥락막비후가 있던 원발개방각녹내장 환자에서 아메드밸브삽입술을 시행한 후 발생한 저안압과 관련된 황반하 장액망막박리를 경험하였기에, 이를 보고하고자 한다.
증례보고
원발개방각녹내장으로 진단받고 치료 중이던 77세 남자 환자가 최대약물치료에도 조절되지 않는 안압과 시야 감소를 주소로 방문하였다. 과거력상 환자는 당뇨가 있었고, 13년 전 타병원에서 좌안에 백내장제거술 및 인공수정체삽입술을 시행받았고, 7년 전 본원에서 좌안에 섬유주절제술을 시행받은 과거력이 있었다. 섬유주절제술 후 환자는 본원에서 경과 관찰을 하지 않았고, 이후 다시 방문하였다.
환자가 다시 방문한 당시 세극등현미경검사에서 전방을 가득 채운 유리체가 관찰되었고, 최대약물치료에도 불구하고 좌안 안압은 골드만압평안압계로 32 mmHg였고, 최대교정시력은 0.32였다. 안저검사에서 좌안의 수직유두함몰비는 0.96으로 증가되어 있었고, 안축장 길이는 22.83 mm였다. 중심전방깊이는 중심각막두께의 5배였다. 빛간섭단층촬영검사에서 시신경 주위 망막신경섬유층과 황반부 신경절세포/내망상층 두께의 감소가 관찰되었다. Humphrey Field Analyzer (Carl Zeiss Meditec Inc, Dublin, CA, USA)의 24-2 SITA standard 측정법으로 시행된 시야검사에서 visual field index는 34%, mean deviation은 -21-92 dB, pattern standard deviation은 9.64 dB이었고, 중심시야와 상이측 시야 일부분만 남아 있었다(Fig. 1A-C). 세 번의 연속된 외래 방문 시에 시행한 파장가변 빛간섭단층촬영(DRI-OCT Triton, Topcon Medical Systems, Oakland, NJ, USA)에서 좌안 중심소와 아래 맥락막두께는 약 510 µm였다. 맥락막의 두께 증가와 함께 맥락막혈관의 확장이 관찰되었고, 황반부 감각신경망막은 정상 형태였다(Fig. 2A, B).
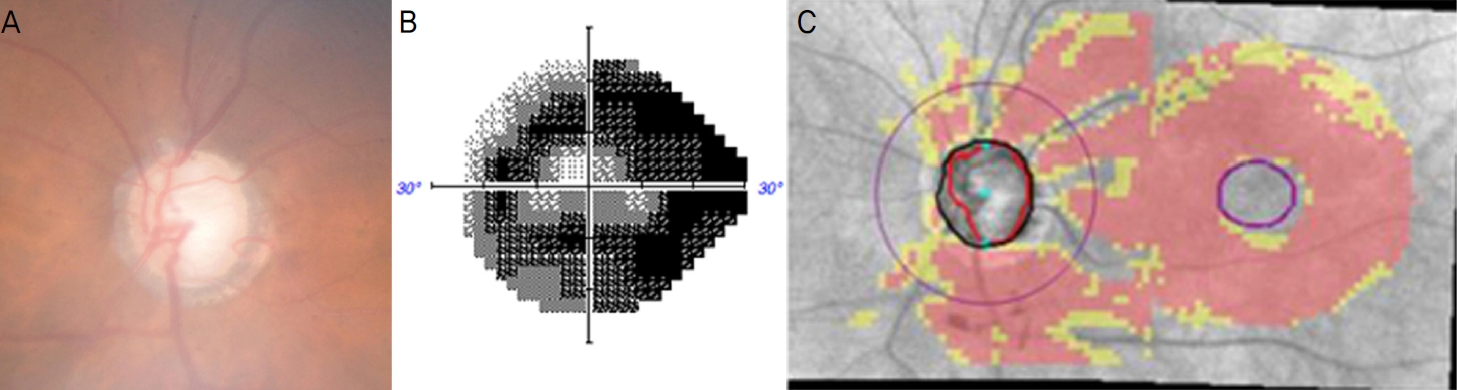
The glaucoma severity of the left eye. (A) Fundus photography showed that vertical cup-to disc ratio increased to 0.96. (B) Standard automated perimetry showed that visual field index, mean deviation, and pattern standard deviation was 34%, -21.92dB, and 9.64dB, respectively. (C) Cirrus optical coherence tomography showed diffuse circumpapillary retinal nerve fiber layer atrophy and macular ganglion cell/inner plexiform layer loss.
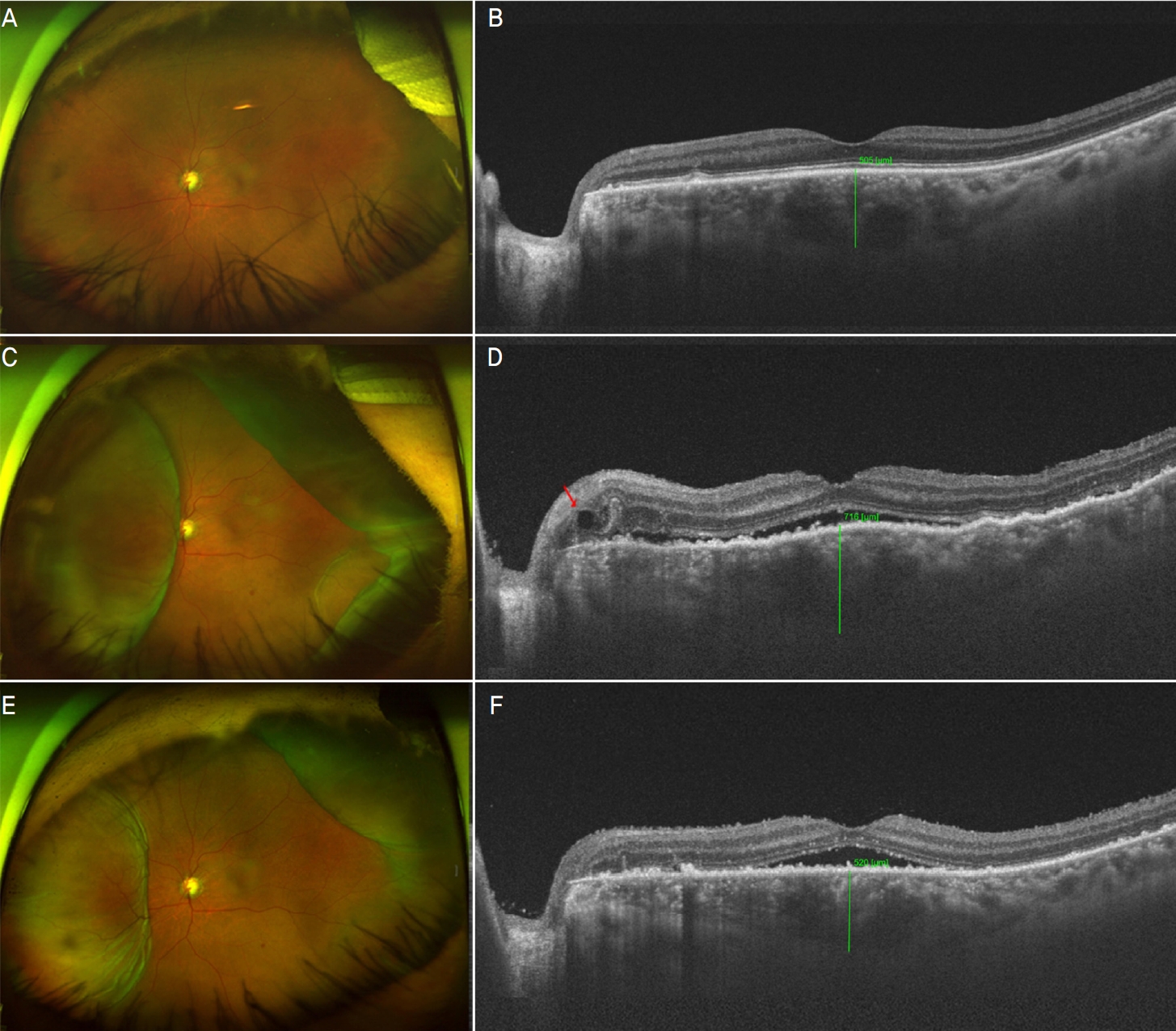
Baseline and postoperative findings of color fundus photography and optical coherence tomography (choroidal thickness is shown). (A) Wide fundus photograph at baseline visits before vitrectomy. (B) Subfoveal choroidal thickness was about 510 μm in swept source-optical coherence tomography (SS-OCT) at baseline. (C) Ten days after Ahmed valve implantation when the intraocular pressure (IOP) of the left eye was 3 mmHg. Choroidal detachment was seen in the wide fundus photograph. (D) Shallow serous retinal detachment with choroidal folding, subretinal precipitates, intraretinal cyst near the optic disc (red arrow), and aggravated pachychoroid (subfoveal thickness was about 720 μm) were observed in SS-OCT. (E) Choroidal detachment showed some decrease 4 days after partial ligation of Ahmed valve tube in wide fundus photograph when the IOP was 15 mmHg. (F) Range of serous retinal detachment showed decrease.
녹내장수술을 계획하고, 녹내장수술 전 전방 내로 탈출된 유리체의 감돈, 유리체의 견인에 의한 망막열공 등을 방지하기 위해 유리체절제술을 먼저 시행하기로 하였다. 유리체절제술 후 2주에 골드만압평안압계로 측정한 좌안의 안압은 19 mmHg였으나, 술 후 3주에는 최대약물치료에도 불구하고 안압이 32 mmHg로 상승하여, 유리체절제술 후 4주에 좌안에 아메드밸브삽입술을 시행하였다.
아메드밸브삽입술 후 1일째 안압은 9 mmHg였으나 술 후 10일째에 안압이 3 mmHg로 감소하여 저안압이 발생하였고 최대교정시력 또한 0.16으로 저하되었다. 광각안저촬영검사에서 맥락막박리가 관찰되었고, 파장가변 빛간섭단층촬영검사에서 중심소와 아래 맥락막두께는 약 720 µm로 측정되었고, 공막과 맥락막의 경계 부위를 정확하게 구별하기 어려울 정도로 맥락막비후는 더 악화되었다. 맥락막의 주름, 시신경의 이측으로부터 황반부를 포함한 부위에 완만한 장액망막박리, 황반하 침착물이 관찰되었고, 시신경유두 주변으로 망막 내 작은 낭포가 발견되었다(Fig. 2C, D).
아메드밸브삽입술 후 17일째까지 시력저하가 지속되었고 중심전방깊이는 2.5 각막두께로 감소하였다. 저안압을 적극적으로 치료하기 위해 아메드벨브삽입술 후 18일째, 아메드밸브의 실리콘 튜브를 8-0 Vicryl suture와 7-0 Prolene suture를 이용하여 부분 결찰술을 시행하였다(Fig. 3A, B).11 튜브 부분 결찰술 후 1일째 안압은 21 mmHg로 증가하였고, 맥락막박리는 호전되기 시작하였다. 튜브 부분 결찰술 후 4일째 골드만압평안압계로 측정된 안압은 15 mmHg로 증가하여 저안압이 호전되었고, 장액망막박리의 범위가 감소하였다(Fig. 2E, F). 튜브 부분 결찰술 11일째 안압은 18 mmHg였고, 장액망막박리는 황반부에 여전히 일부 남아 있는 양상을 보였으나 중심소와 아래 맥락막두께는 580 µm 정도로 감소하여 맥락막비후가 튜브 부분 결찰술 이전보다 개선되었다(Fig. 4A, B). 튜브 부분 결찰술 후 6주째 안압은 14 mmHg로 유지되었고, 최대교정시력은 0.5로 호전되었다. 황반하 장액망막박리가 파장가변 빛간섭단층촬영검사에서 사라진 것이 관찰되었고, 중심소와 아래 맥락막두께는 약 510 µm로 감소하였다(Fig. 4C, D). 아메드밸브삽입술 후 5개월째에 파장가변 빛간섭단층촬영검사에서 맥락막 비후는 여전히 관찰되었으나, 망막하액은 재발하지 않았다(Fig. 4E, F). 교정시력은 0.5로 호전되어 유지되었다.

Ahmed valve tube partial ligation was performed on 18 days after Ahmed valve implantation (A, B).
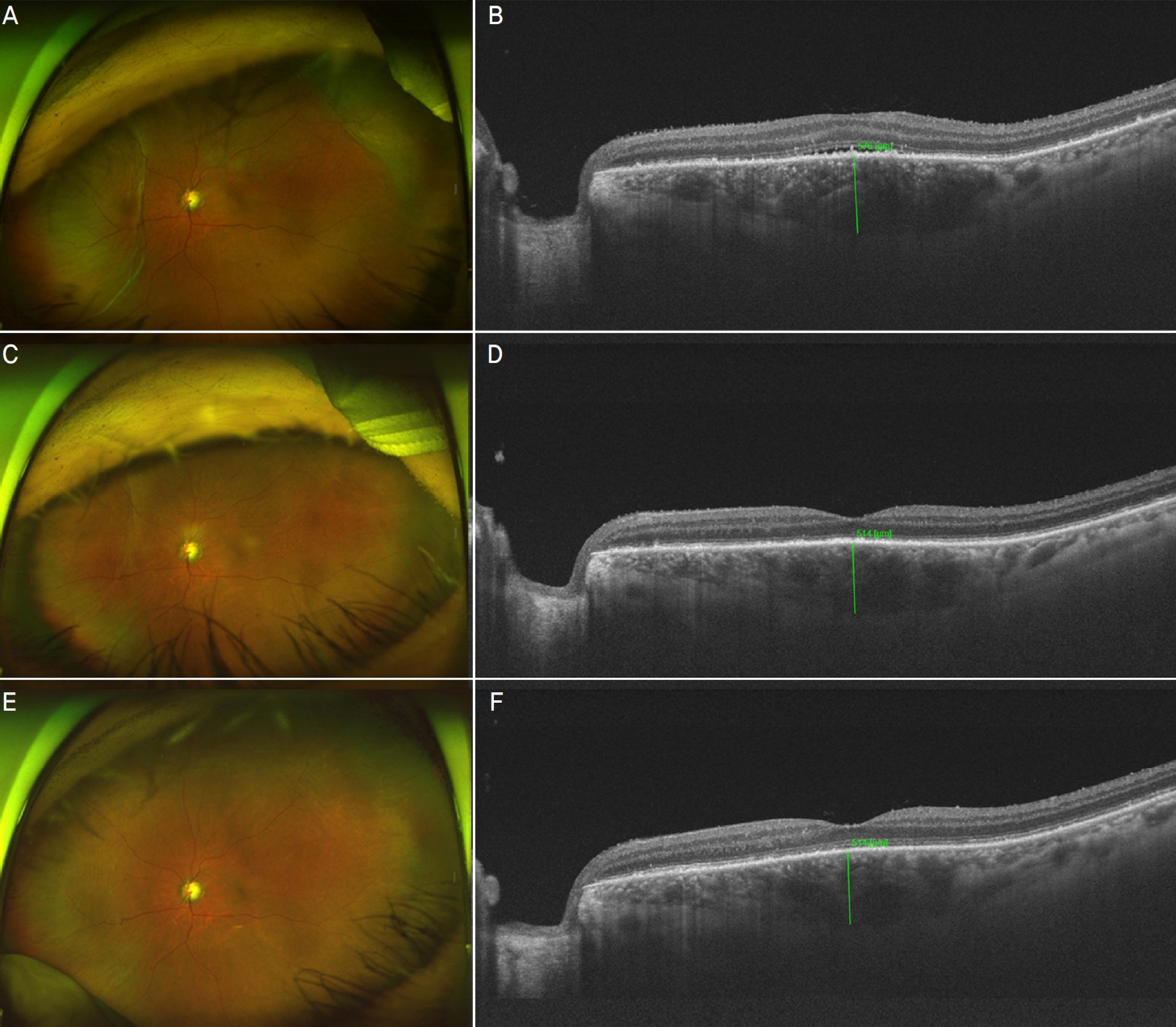
Changes in choroidal detachment, choroidal thickness, and serous retinal detachment observed in fundus photography and optical coherence tomography (choroidal thickness is shown). (A) Wide fundus photograph at 11 days after the tube partial ligation when the intraocular pressure (IOP) was 18 mmHg. (B) Subretinal fluid was still seen, but choroidal thickness showed some decrease (subfoveal thickness = 580 μm) in swept source-optical coherence tomography (SS-OCT). (C) Wide fundus photography at 6 weeks after the tube partial ligation when IOP remains around 14 mmHg and the visual acuity increased. (D) Subfoveal choroidal thickness decreased to about 510 μm. (E) Wide fundus photography at 5 months after Ahmed valve implantation. (F) Fovea remained attached and no precipitation was found in SS-OCT while pachychoroid was still seen.
고 찰
Kokame et al8은 만성 포도막염을 가진 39세 여자 환자에게서 Baerveldt 임플란트삽입술 후 발생한 저안압에서 황반부 장액망막박리가 낭포황반부종과 동반된 증례를 보고한 바 있다. Shimokawa et al9은 낭포황반부종이 없는 장액망막박리가 저안압과 연관되어 생긴 두 개의 증례를 보고하였다. 첫 번째 증례는 66세 여자 환자에게서 발생한 당뇨와 연관된 신생혈관녹내장의 증례로, 이전에 당뇨망막증으로 범망막광응고술, 유리체절제술, 유리체강 내 트리암시놀론 주입술을 시행받은 적이 있으며 섬유주절제술을 시행받은 후 안압이 8 mmHg로 감소하면서 황반부 장액망막박리가 발생하였다. 술 전에 시행한 파장가변 빛간섭단층촬영검사에서는 맥락막두께가 정상이었으나 술 후 두께가 400 µm 이상으로 증가하였다가 안압이 증가하면서 두께가 다시 감소하여 정상화되었고, 황반부 장액망막박리가 호전되었다. 또 다른 환자는 60세 남자로 당뇨망막병증으로 범망막광응고술, 유리체강 내 트리암시놀론 주입술을 시행받은 적이 있으며 섬유주절제술 후 안압이 3 mmHg로 감소하면서 맥락막비후와 함께 황반부 장액망막박리가 발생한 경우였다. 두 증례는 모두 당뇨망막병증과 관련한 신생혈관녹내장에서 섬유주절제술 후 저안압으로 인해 맥락막망막주름이 발생한 후, 황반부 장액망막박리의 형태로 저안압 황반병증이 발생한 경우이다.
국내 보고에서는 단안의 중심장액성 맥락망막병증 환자에서 반대안의 섬유주절제술 후 중심장액성 맥락망막병증이 발생하였고, 포도막염의 과거력, 섬유주절제술 후 안압 감소, 수술 후 스테로이드의 사용을 원인으로 유추하였다.10 그러나 본 증례와 다르게 맥락막비후가 없었으며, 포도막과 망막의 주름과 같은 저안압 황반병증의 특징적인 소견도 없었고, 수술 후 약 4일간 매일 8 mg의 트리암시놀론을 경구 복용 후 중심장액성 맥락망막병증이 발생하여 섬유주절제술 후 발생한 저안압에 의한 것이라고 보기는 어렵다고 주장하였다.10
본 증례는 위의 보고들과 달리, 기존에 맥락막비후가 이미 존재했던 환자에게서 아메드밸브삽입술 후 발생한 저안압 황반병증이며, 황반부의 장액망막박리와 시신경유두주위 낭포의 형태로 관찰되었다. 또한, 아메드밸브삽입술 후 발생한 저안압 상태에서 맥락막의 두께는 더 증가하면서 황반부 장액망막박리가 관찰되었고, 안압이 오르면서 망막의 병변은 호전되었고 맥락막의 두께는 다시 술 전 수치로 돌아간 경우이다. 다만, 본 증례의 환자에게는 7년 전 섬유주절제술을 시행받은 좌안에만 맥락막비후가 있었는데 맥락막비후가 오래 전에 시행한 섬유주절제술과 관련하여 발생한 것이었는지는 그 전 기록이 남아 있지 않아 확인하기가 어렵다.
맥락막비후가 존재하는 눈에서는 맥락막혈관의 직경이 증가하는 구조적인 변화와 함께 맥락막혈관의 투과성이 증가하는 기능적인 변화가 존재한다.12 즉, 본 증례에서와 같이 맥락막비후가 존재하는 눈에서 저안압이 발생하면, 맥락막 상부 조직의 세포 간 압력이 감소하고 맥락막혈관압이 상대적으로 더 높아지면서 맥락막비후 질환군의 한 형태인 중심장액맥락망막병증과 유사한 장액망막박리가 일어났을 가능성이 있다. 또한, 공막의 형태 변형이 또아리정맥의 혈액 정체에 영향을 주거나 주변 조직에 영향을 미쳐서 맥락막비후가 악화되었을 가능성도 있다.
시신경유두주위 신경망막층 내의 낭포는 시신경유두주위 망막층간분리, 맥락막비후 질환군에서 주로 관찰되는데, 저안압증으로 인해 나타나고, 저안압증이 호전된 후에 사라졌다는 보고가 있다.13 본 증례에서도 저안압증이 호전된 후에 시신경유두주위 낭포는 사라진 것을 관찰할 수 있었다.
아메드밸브삽입술 후 4주 정도가 지나면 아메드밸브 몸체 주위에서 섬유성 캡슐화(encapsulation)가 발생하여 안압이 올라가면서 저안압이 교정될 수 있다.14 그러나 본 증례와 같이 맥락막비후가 있는 눈에서 황반하 장액망막박리는 망막색소상피가 맥락막혈관의 울혈을 극복할 수 없을 정도로 그 기능이 떨어졌거나 손상된 경우에 발생한다.12 저안안 황반병증이 황반하 장액망막박리의 형태로 나타난 경우 시력 예후에 관해서는 잘 알려진 바가 없고, 망막색소상피의 기능적 혹은 구조적 손상이 시력에 미칠 영향을 고려하여,4 저안압을 적극적으로 교정하기 위해 아메드밸브 튜브의 부분 결찰술을 시행하였다.
저안압과 관련된 황반병증은 대부분 맥락막과 망막의 주름과 함께 낭포황반부종의 형태로 나타나고,15 드물게 장액망막박리의 형태로 보고되기도 한다.8 그러나 기존에 맥락막비후가 있는 환자에게서 녹내장수술 후 저안압이 발생하면, 맥락막비후가 악화되면서 황반부 장액망막박리의 형태로 저안압 황반병증이 발생할 수 있다는 점을 고려하여야 하겠다.
Acknowledgements
This work was supported by a 2-year Research Grant of Pusan National University.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.
References
Biography
김은아 / EunAh Kim
부산대학교 의과대학 안과학교실
Department of Ophthalmology, Pusan National University School of Medicine
