눈 매독에 동반된 견인 망막박리 1예
A Case of Traction Retinal Detachment Accompanied by Ocular Syphilis
Article information
Abstract
목적
국내에 보고된 적 없는 눈 매독에 동반된 견인 망막박리 1예를 경험하여 보고하고자 한다.
증례요약
20세 남자 환자가 좌안 시력저하를 주소로 내원하였다. 최대교정시력은 0.3이었고 전방 내 염증 소견은 없었으나 유리체내 염증세포가 다수 확인되었다. 안저검사상 삼출성 망막박리가 아래쪽에서 발견되었고 빛간섭단층촬영에서 황반부 망막앞막이 확인되었다. 플루레신조영촬영에서는 망막박리 부위에 초기와 후기 모두 저형광 소견을 보였다. 혈청검사상 매독이 확인되어 ceftriaxone 2 g 정맥내 주사를 14일간 시행하였다. 이후 유리체내 염증은 호전되었으나 견인 막이 증식하면서 견인 망막박리가 나타나 유리체절제술, 견인 막 제거술, 유리체강 내 항생제주입술을 시행하였다. 이후 14일 동안 penicillin G 20 MU정맥 내 주사 후 퇴원하였다. 유리체절제술 3달 후 외래 내원 시 최대교정시력은 0.8로 호전되었고 견인 망막박리의 재발은 관찰되지 않았다.
결론
눈 매독 환자에서 전신 항생제 치료에도 불구하고 망막박리가 생길 수 있다. 수술적 치료의 가능성을 염두에 두어야 하며 적절한 시기에 유리체절제술을 시행하여 좋은 결과를 얻을 수 있다.
Trans Abstract
Purpose
We report a first case of traction retinal detachment accompanied by ocular syphilis in Korea.
Case summary
A 20-year-old male visited with poor left-eye vision. His best-corrected visual acuity was 0.3; no inflammation was evident in the anterior chamber, but many inflammatory cells were found in the vitreous cavity. Fundus examination revealed inferior exudative and tractional retinal detachment. Optical coherence tomography revealed an epiretinal membrane; fluorescein angiography showed that the inferior (detached) retina did not fluoresce. Syphilis was serologically detected; ceftriaxone (2 g daily) was intravenously injected for 14 days. The vitreous cavity inflammation improved, but the tractional membrane proliferation triggered tractional retinal detachment. We performed vitrectomy to remove the tractional membrane and prescribed intravitreal antibiotics. The patient was discharged after intravenous injection of penicillin G (20 MU daily) for 14 days. Three months after surgery, the best-corrected left-eye visual acuity had improved to 0.8, and no recurrence of the retinal detachment was noted.
Conclusions
Patients with ocular syphilis may evidence retinal detachment despite initial prescription of systemic antibiotics. A possible need for surgery should be kept in mind; the prognosis is good if an operation is performed in a timely manner.
매독은 Treponema pallidum이라는 Spirochete에 의해 감염되는 성매개질환으로 전신 장기에 침범하고 눈 염증을 일으킬 수 있다[1]. 임상 소견은 매우 다양하여 결막, 공막, 각막, 수정체, 포도막, 망막, 망막혈관, 시신경, 동공 운동신경 전달 경로, 외안근을 조절하는 뇌신경계 등을 침범할 수 있으며 매독의 어떤 단계에서든지 발생할 수 있다[2]. 임상 소견 중 가장 흔한 것은 포도막염으로 전안부, 후안부 혹은 양쪽 부위 모두에서 발생할 수 있으며 중간포도막염의 양상을 보이기도 한다. 앞포도막염에 동반되는 소견에는 홍채 결절, 확장된 홍채 혈관, 홍채 위축, 홍채 후부 유착, 수정체 탈구 등이 있고, 뒤포도막염에서 흔한 양상은 유리체 염증, 망막혈관염, 맥락망막염, 시신경염, 장액성 망막박리 등이 있다[3,4]. 눈 매독에 대해 확립된 치료법은 없으나 가능한 빠른 시기에 매독균에 대해 항생제 치료를 시작하는 것이 치료에 있어 가장 중요하다. 일반적으로 감염내과 전문의와 협진하여 penicillin G 18-24 MU을 10-14일 동안 정맥 내로 주사한다[5]. 저자들은 최근 눈 매독에서 전신 항생제 치료 후 염증이 호전되었으나 합병증으로 견인 망막박리가 동반된 1예를 경험하였다. 눈 매독에서 견인 망막박리가 동반된 사례는 국내에서 보고된 바가 없기에 이를 보고하고자 한다.
증례보고
기저질환이 없는 20세 남성이 16주 전 시작된 좌안 시력 저하로 내원하였다. 내원 당시 최대교정시력은 우안 1.0, 좌안 0.3이었고 안압은 정상 범위에 있었다. 세극등현미경검사에서 양안 전방내 염증세포는 없었고, 좌안 유리체내 염증세포가 4+로 확인되었다. 안저검사에서 좌안 망막 하부에서 삼출에 의한 망막박리가 관찰되었고, 빛간섭단층촬영에서 좌안 망막앞막이 확인되었다. 형광안저혈관조영에 서 좌안 망막 하부의 저형광 소견이 있었다(Fig. 1, 2). 눈 매독을 감별하기 위해 혈청을 채취하여 시행한 FTA-ABS IgM, VDRL (venereal disease research laboratory) 검사에서 비반응성 결과가 나왔으나 treponema pallidum hemagglutination assay 검사에서 양성 결과가 나왔다. 감염내과 전문의와 협진하에 ceftriaxone 2 g 정맥내 주사를 14일 동안 시행하였다. 국소점안제로는 0.5% moxifloxacin hydrochloride (Moroxacin eye drops; Hanmi Pharm., Seoul, Korea) 점안액과 1% prednisolone acetate (Prednilone eye drops; Dae Woo Pharm., Seoul, Korea) 점안액을 사용하였다.
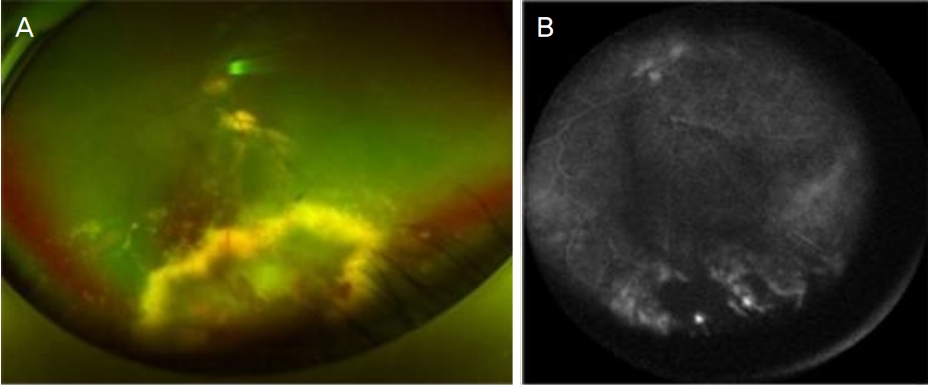
Fundus examination of the left eye at first visit. (A) Color fundus photograph revealed inferior exudative and tractional retinal detachment. (B) Fluorescein angiography showed that the inferior (detached) retina did not fluoresce. A few leaking points were detected in late stage on fluoresceine angiography.
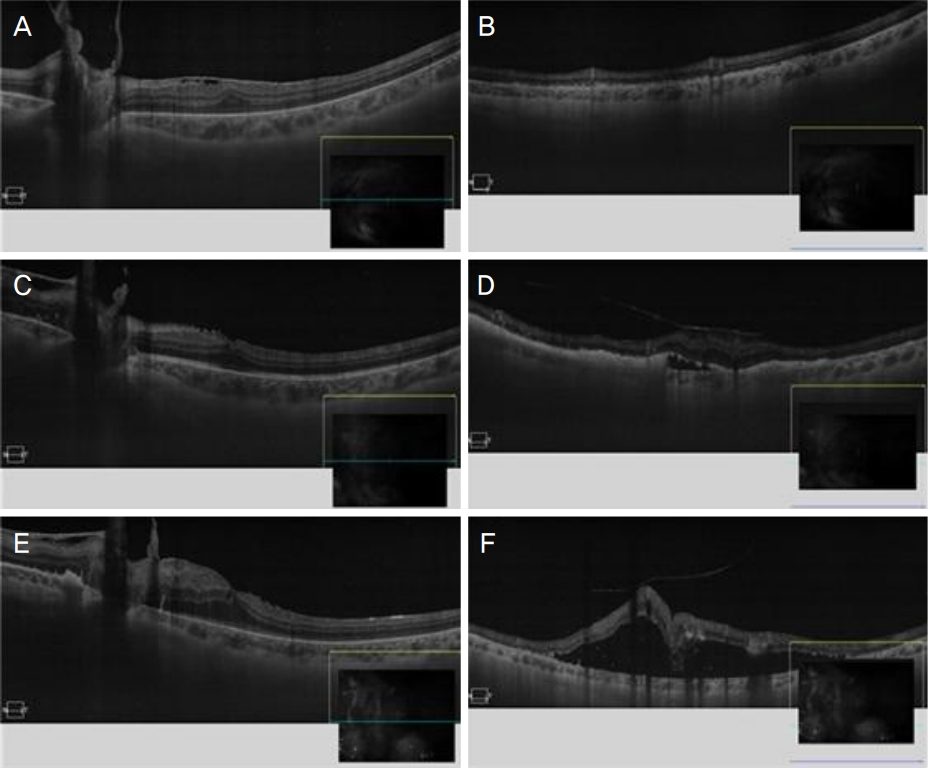
Optical coherence tomography of the left eye. The first visit (A, B) and 20 weeks (C, D), 30 weeks (E, F) after the first visit. (A) Epiretinal membrane was found near the macula. (B) Hyperreflective deposit was found under neurosensory retina in the inferior part of attached retina. (C) Epiretinal membrane disappeared near the macula, but (D) in the inferior part of retina, epiretinal membrane acted as tractional membrane and neurosensory retina was pulled by it. (E) Epiretinal membrane was aggravated and the posterior pole was distorted by tractional membrane. (F) Retinal detachment occured beneath the detached neurosensory retina and thick epiretinal tractional membrane.
Ceftriaxone 정맥내 주사 치료 20주 뒤 좌안 최대교정시력은 0.4로 측정되었고 좌안 유리체내 염증세포는 2+로 호전되었으나 기존에 있던 좌안 망막앞막에 증식막이 늘어나 두꺼운 견인 막이 형성되어 망막을 당기는 소견이 관찰되었다. Ceftriaxone 정맥내 주사 치료 30주 뒤 좌안 유리체내 염증세포는 2+로 변화 없었으나 좌안 망막하액이 증가하고 견인 망막박리가 진행하는 소견을 보여(Fig. 2) 유리체절제술, 견인 막 제거술, 유리체강내 항생제(ceftazidime 2.25 mg/0.1 mL) 주입술을 시행하였다. 동시에 수술 하루 전부터 penicillin G 2.0 MU 정맥내 주사를 14일동안 매일 시행하였다.
유리체절제술 12주 후 최대교정시력은 우안 1.0, 좌안 0.8로 호전되었다. 유리체내 염증세포는 1+로 관찰되었고, 망막하 삼출액은 감소하였으며 견인 망막박리 재발이 의심되는 소견은 관찰되지 않았다(Fig. 3).
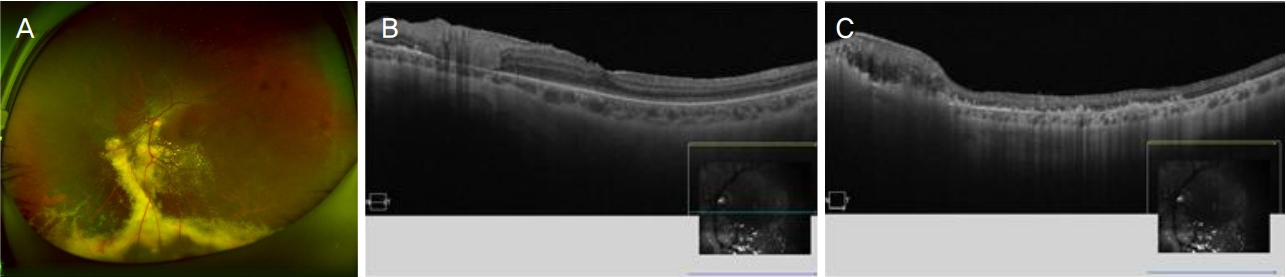
Color fundus photograph and optical coherence tomography of left eye at 12 weeks after surgery. (A) Retina was attached well and exudates remained in the inferior part of retina. (B) Epiretinal membrane was well removed and not recurred. (C) Retina was attached well and subretinal fluid was absorbed in the inferior part of retina. But atrophic change progressed on detached region of the retina.
고 찰
매독과 마찬가지로 눈 매독의 표준 치료는 penicillin G 18-24 MU 정맥내 주사 치료로 알려져 있다[5]. Mathew et al [6]에 따르면 2009년부터 2011년 사이 모집된 41예의 눈 매독 환자들(63예의 안구) 중 92.1%가 penicillin G 정맥내 주사 치료 후 20/40 이상의 양호한 시력 예후를 얻었다. 이처럼 눈 매독은 penicillin G 정맥내 주사 치료만으로 좋은 예후를 보인다. 하지만 일부에서 망막박리가 동반되어 결과가 좋지 못한 사례도 제시되고 있다.
Jumper et al [7]에서 연구한 매독 포도막염 환자 3예에서 모두 삼출성 망막박리가 동반되었고 유리체강내 penicillin 주입술 후 망막박리는 호전되었으나 시력예후는 좋지 못했다. 또한 Queiroz Rde et al [8]의 매독 포도막염 19예 중 4예에서 견인-열공 망막박리와 증식성 유리체 망막병증이 동반되었는데, 이들은 모두 penicillin G 정맥내 주사 치료를 받았음에도 망막박리가 진행되었다. 이 중 2예에서는 망막박리에 대해 수술적 치료를 시행하였는데 수술 도중 채취한 망막앞막의 조직검사상 섬유아교조직, 신경아교세포, 망막색소상피 화생과 함께 림프구, 형질세포 등의 염증세포가 확인되었다. 이를 통해 눈 매독에서 견인 막이 생기는 원인으로, 눈 속 염증에 의해 분비된 성장인자(platelet derived growth factor, fibroblast growth factor, tumor necrosis factor [TNF]-α, TNF-β)와 cytokine (interleukin [IL]-1, IL-6, IL-8, IL-10, interferon-γ)이 세포 이동과 증식을 일으켜 증식막이 형성되는 것으로 생각해볼 수 있다[8].
본 증례에서는 초기에 점안용 스테로이드 제제를 사용하였고 혈청검사에서 매독이 검출되자마자 전신 항생제 치료를 시작하였다. 매독의 표준 치료로 알려진 penicillin G는 국내에서 희귀의약품으로 분류되어 있으며 한국희귀필수 의약품센터를 통한 구입 절차에 시간이 소요되므로, 우선 penicillin G를 대신하여 ceftriaxone 2 g 정맥내 주사 치료를 시행하였다. Ceftriaxone은 최근 매독에서 penicillin G를 대신해 사용되는 항생제로 중추신경계 침투력이 좋고 반감기가 7시간으로 길다[9]. 또한 하루 1 g의 정맥주사 용량으로 트레포네마 균의 최소 저지 농도(minimum inhibitory concentration) 수치인 0.0006 μg/mL에 도달할 수 있다[10]. Shann and Wilson [11]은 신경매독 환자 1예에서 14일 동안 ceftriaxone 1 g 정맥내 주사 치료를 시행하였고 1:128이었던 혈중 RPR (rapid plasma reagin) 수치가 36개월 뒤 추적 관찰에서 1:16으로 호전되는 결과를 얻었다. 또한 Marra et al [9]은 후천성 면역 결핍증을 동반한 신경매독 환자 30예를 cefriaxone 정맥내 주사 치료를 받은 14dP와 penicillin G 정맥내 주사 치료를 받은 16예로 나누어 비교하였는데, 치료 14-26주 뒤 뇌척수액내 백혈구 수, 단백질 농도, VDRL 역가는 큰 차이를 보이지 않았으나 혈중 RPR 역가에서 ceftriaxone으로 치료받은 군의 경과가 월등히 좋았다고 보고하였다.
본 증례에서는 ceftriaxone 정맥내 주사 치료 이후 유리체 내 염증은 호전을 보였고 좌안 교정시력이 0.4로 양호한 편이었으며 젊은 나이, 수술 후 재발 가능성 등을 고려하여 경과 관찰하였다. 하지만 망막의 견인 막은 점차 증식하여 견인 망막박리가 발생하였다. 망막박리의 진행을 막고 박리된 망막을 유착시키기 위해 유리체절제술을 시행하였다. Sood et al [12]에 따르면 눈 매독은 Treponema pallidum이 혈액을 통해 눈에 전파된 것으로 내인성 세균성 안내염의 형태로 생각할 수 있으며, 안내염과 마찬가지로 안내 항생제 주입술 치료를 시행해볼 수 있다. Sood et al [12]은 penicillin에 대한 과민 반응이 있는 45세 눈 매독 환자에서 penicillin에 대해 탈감작을 하는 기간 동안 양안에 유리체강내 ceftazidime (2.25 mg/0.1 mL) 주입술을 시행하였고 하루 뒤 망막의 염증은 눈에 띄게 호전되었다고 보고하였다. 또한 Lim et al [13]은 후천성 면역결핍증을 동반한 눈 매독 환자 3명에게 유리체강내 ceftazidime (1.125 mg/0.05 mL) 주입술을 시행하였고 3예 모두 시력과 염증 완화에서 좋은 예후를 보였다고 보고하였다. 저자들은 위 증례들을 참조하여 유리체절제술 시 유리체강내 ceftazidime (2.25 mg/0.1 mL) 주입술을 시행하였고 penicillin G 2.0 MU 정맥내 주사와 병행하여 좋은 결과를 얻었다.
Sood et al [12], Lim et al [13]은 눈 매독 환자의 치료 과정에서 penicillin 정맥 내 주사, 유리체강내 ceftazidime 주입술 그리고 경구 steroid 제제를 병용하여 좋은 결과를 얻었다 보고하였는데, 본 증례에서는 신경매독 악화를 우려하여 steroid 제제를 사용하지 않았으나 병용했었다면 삼출액 증가, 견인 막 악화 등 염증성 반응 조절 효과를 통해 조금 더 나은 결과를 얻을 수도 있지 않았을까 생각한다. 또한 치료 초기 단계에서 유리체강내 ceftazidime 주입술을 바로 시행했다면 치료 결과에 도움이 될 수 있지 않았을까 생각한다[12,13].
본 증례의 환자는 증상이 생긴지 16주째에 내원하였다. 당시부터 좌안 망막에서 삼출에 의한 망막박리와 망막앞막이 확인되었다. 내원 당시 이미 눈 매독이 상당히 진행된 상태였으므로 진단 직후 치료에도 불구하고 견인 막이 발생하여 망막박리로 진행한 것이라 추측해볼 수 있다. 눈 매독 환자에서 조기 진단과 빠른 치료가 중요하며 수술적 치료 가능성 또한 염두에 두어야 한다. 특히 증상 발생 후 시간이 경과되고 진단 시점이 늦은 경우 망막표면에 증식막이 동반되면 적절한 항생제와 항염증 치료에도 불구하고 견인 망막박리가 진행할 수 있으므로 환자 상태를 자주 관찰하여 수술적 치료가 지연되지 않도록 주의해야 한다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
허정우 / Jeong Woo Heo
동아대학교 의과대학 안과학교실
Department of Ophthalmology, Dong-A University College of Medicine
