젠 스텐트 삽입술 후 발생한 스트렙토코커스 인판타리우스 안내염
Streptococcus infantarius Endophthalmitis after XEN Gel Stent Implantation
Article information
Abstract
목적
XEN® Gel Stent와 관련된 Streptococcus infantarius 안내염을 치료한 경험이 있어 이를 보고하고자 한다.
증례요약
75세 남자 환자가 원발개방각녹내장으로 좌안 XEN® Gel Stent 삽입술을 받은 후 55일째 발생한 안내염으로 본원으로 전원되었다. 시력은 20/50이었다. 세극등현미경검사에서 결막충혈, 전방염증과 축농이 관찰되었으며, 안저에서 유리체내 염증과 삼출성막이 관찰되었다. XEN® Gel Stent 제거술, 전방세척술, 전방 및 유리체강내 항생제 주입술, 방수 배양검사를 시행하였다. 시행한 배양 검사에서 Streptococcus infantarius가 동정되었다. 술 후 5일째 시력이 안전수동으로 감소하고 염증이 악화되어 추가적인 유리체절제술, 전방세척술, 유리체강내 항생제 주입술을 시행하였다. 유리체절제술 후 16일째 전방염증이, 34일째 맥락막박리가 모두 호전되었다. 술 후 6개월까지 염증은 재발 없이 유지되었으나 시력은 20/100으로 회복에 제한이 있었다.
결론
XEN® Gel Stent 삽입술 후 발생한 세균성 안내염에서 방수유출장치를 제거하고 유리체절제술과 안내 항생제 치료를 통해 성공적으로 치료가 가능하였다.
Trans Abstract
Purpose
To report a case of Streptococcus infantarius endophthalmitis related to the use of a XEN® Gel Stent.
Case summary
A 75-year-old male was referred to our practice with a diagnosis of endophthalmitis 55 days after XEN® Gel Stent implantation. He had primary open-angle glaucoma. Visual acuity was 20/50. Slit-lamp examination revealed conjunctival injection and anterior chamber inflammation with hypopyon. Fundus examination showed inflammatory cells with exudative materials in the vitreous. The aqueous sampling for culture of causative micro-organisms was followed by removal of the XEN® Gel Stent, along with anterior chamber irrigation and intracameral and intravitreal injection of antibiotics. Streptococcus infantarius was isolated after 5 days. Vitrectomy, anterior chamber lavage, and intravitreal injection of antibiotics were additionally performed to control the intraocular inflammation. Sixteen days after vitrectomy, the intraocular inflammation disappeared. The choroidal detachment was resolved 34 days after vitrectomy. Visual improvement was limited to 20/100 at 6 months.
Conclusions
XEN® Gel Stent-related bacterial endophthalmitis was successfully treated by implant removal, vitrectomy, and proper intraocular antibiotic treatment.
최소침습 녹내장수술(minimally invasive glaucoma surgery, MIGS)은 결막 및 공막의 조작과 손상을 최소화하고, 수술 후 방수유출의 높은 안전성과 빠른 회복 기간을 기대할 수 있는 수술이다[1]. XEN® Gel Stent (Allergen, Dublin, CA, USA)는 2016년 FDA 승인을 받은 후 현재 임상에서 널리 사용 중인 새로운 MIGS로, 돼지 피부의 젤라틴 성분으로 구성된 친수성의 스텐트를 전방에서부터 결막아래 공간으로 삽입하여 방수유출을 도와 안압을 하강시키는 녹내장수술이다[1,2]. 이전 임상연구들에서는 XEN® Gel Stent 삽입술 후 전방출혈, 저안압, 전방 얕아짐, 스텐트 위치이상, 여과포 누출 등의 합병증이 발생한 경우는 보고된 바 있으나 안내염과 같은 심각한 안구 합병증에 대한 국내 보고는 아직 없다[3,4]. 하지만 XEN® Gel Stent도 일종의 방수유출장치이므로 기존의 수술과 동일한 다양한 합병증이 발생할 수 있다. 특히, 스텐트를 통해 결막아래 공간으로 유출된 방수가 여과포를 형성하게 되므로, 여과포 관련 안내염 같은 심각한 합병증이 발생 가능하며 적절한 치료가 동반되지 않으면 심한 시력소실을 경험하게 될 수 있다. 저자들은 XEN® Gel Stent 삽입술 후 발생한 안내염을 성공적으로 치료하였기에 이를 보고하고자 한다.
증례보고
75세 남자 환자가 원발개방각녹내장으로 개인의원에서 좌안 XEN® Gel Stent 삽입술을 받은 후 55일째 되는 날 발생한 통증과 결막충혈, 시력저하가 발생하여 안내염 진단 하 본원으로 전원되었다. 전신질환은 없었다. 내원 당시 시력은 20/50, 안압은 12 mmHg였다. 세극등현미경검사에서 결막충혈, 전방내 염증세포(4+)와 축농이 관찰되었으며(Fig. 1A), 안저에서 유리체내 염증세포(+3)와 삼출성 막이 관찰되었다(Fig. 1B). 내원 당일 XEN® Gel Stent 제거술, 전방세척술, 전방 및 유리체강내 항생제주입술, 방수 배양검사를 시행하였다.
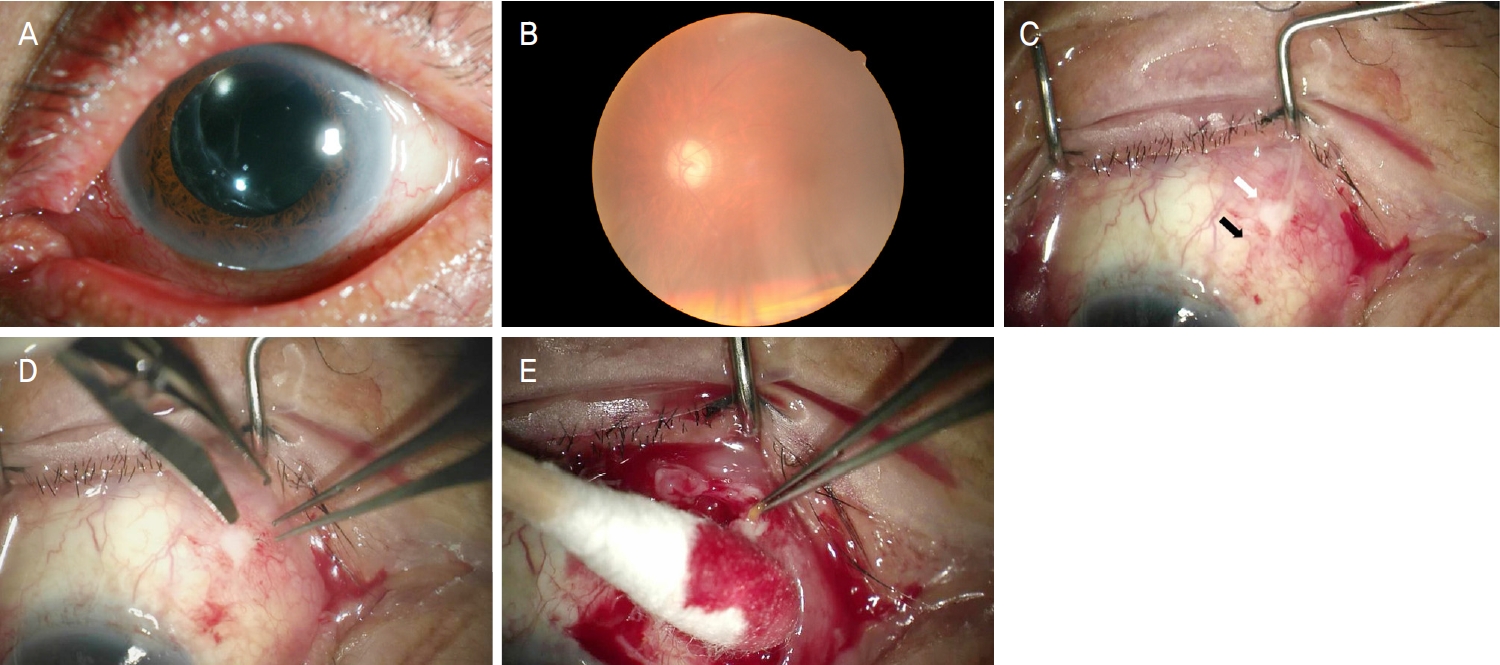
Anterior segment and fundus photographs at the baseline. (A) The conjunctival injection and inflammatory cells were observed in the anterior chamber. (B) Fundus was blurry visible. (C) XEN® Gel Stent (Allergen, Dublin, CA, USA) was located under the subconjunctival space (black arrow). Mucopurulent pus leaked from the bleb (white arrow). (D) One suture was observed behind the pus. (E) XEN® Gel Stent was removed using the tooth forceps.
수술 방법은 먼저 각막견인봉합을 시행하여 안구를 아래쪽으로 주시하게 하고 상비측에 형성된 여과포를 검사하였다. 무혈관성 여과포에서 화농성 농의 누출이 관찰되었다(Fig. 1C). 이전 수술 후 남겨진 봉합사를 제거한 뒤(Fig. 1D) 여과포와 그 주변의 결막을 절제하고 농을 제거한 후 결막과 테논낭을 박리해 가면서 XEN® Gel Stent를 찾았다. 결막아래 테논낭 부위에 섬유화된 조직 속에서 이식된 XEN® Gel Stent가 발견되었다(Fig. 1E). XEN® Gel Stent는 각막 윤부 3 mm 뒤에서 전방으로 삽입되어 있었다. 조심스럽게 XEN® Gel Stent를 집게로 집어 빼내었다. XEN® Gel Stent 속에도 화농성 농이 있었다. 전방천자를 통해 채취된 방수와 제거된 XEN® Gel Stent를 균 배양검사를 위하여 함께 의뢰하였다. 이후 전방을 vancomycin HCl 100 mg/2 mL를 섞은 평형염액(balanced salt solution)으로 세척하였다. 결막을 봉합한 뒤 전방내 항생제(vancomycin HCl 1.0 mg/0.1 mL)와 유리체강내 항생제(vancomycin HCl 1.0 mg/0.1 mL, ceftazidime 2.0 mg/0.1 mL)를 주입하고 수술을 종료하였다.
술 후 1일째 시력은 안전수동, 안압은 26 mmHg였으며, 세극등현미경검사에서 결막충혈, 각막부종, 전방의 염증세포(4+)와 축농, 삼출성 막이 관찰되었다. 국소 점안제로 fortified vancomycin HCl 25 mg/mL과 fortified ceftazidime 50 mg/mL을 매시간마다 점안하고, cyclopentolate hydrochloride (Ocucyclo®, Samil Pharm., Seoul, Korea)를 하루 2회 점안하였다. 또한 dexamethasone (Maxidex®, Norvatis Korea, Seoul, Korea) 점안액을 하루 4회, dexamethasone/neomycin sulfate/polymyxin B sulfate (Forus®, Samil Co., Ltd., Seoul, Korea) 연고를 자기 전 1회 점안하였다. 술 후 2일째 시력은 안전수동, 안압은 6 mmHg였다. 술 후 2일, 4일째 추가적인 유리체강내 항생제(vancomycin HCl 1.0 mg/0.1 mL, ceftazidime 2.0 mg/0.1 mL) 주입술을 시행하였다. 술 후 4일째 술 중 시행한 배양검사에서 Streptococcus infantarius subsp. Infantarius가 동정되었고, 항생제 감수성 검사에서는 penicillin, ampicillin, cefotaxime, ceftriaxone, clindamycin, linezolid, tetracyclin, vancomycin 등에 감수성이 있는 것으로 나타났다. 술 후 5일째 XEN® Gel Stent가 삽입되어 있던 결막 부위 염증은 더 이상 관찰되지 않았으나(Fig. 2A), 전방의 염증세포(4+)와 축농이 감소되지 않아(Fig. 2B) 추가적인 유리체절제술, 전방세척술, 유리체강내 항생제(vancomycin HCl 1.0 mg/0.1 mL) 주입술을 시행하였다. 수술 중 안저에서 맥락막박리가 관찰되었다.
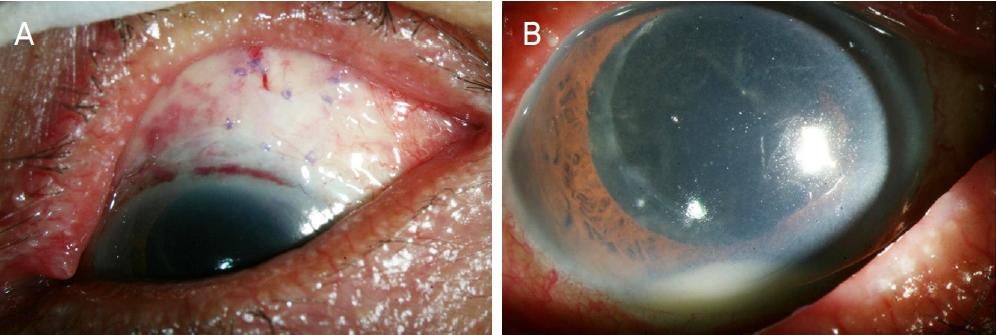
Anterior segment photographs 5 days after removal of XEN® Gel Stent (Allergen, Dublin, CA, USA). (A) The pus disappeared at the lesion of previous XEN® Gel Stent. (B) Hypopyon increased.
추가적인 유리체절제술, 전방세척술 후 1일째 전방축농과 유리체혼탁은 관찰되지 않았다. 술 후 점진적으로 눈속 염증과 맥락막박리는 호전되어 16일째에는 시력 20/100, 안압은 13 mmHg였으며, 전방의 염증세포가 관찰되지 않았다. 이후 점안 항생제를 감량하였다. 술 후 34일째 시력은 20/100, 안압은 11 mmHg였으며, 맥락막박리는 모두 호전되었다. 술 후 6개월까지 염증은 재발 없이 안정된 상태가 유지되었으나(Fig. 3A) 시력은 20/100으로 회복에 제한이 있었다. 무혈관성의 여과포가 관찰되었으며(Fig. 3B), 안저는 특이 소견이 없었다(Fig. 3C).
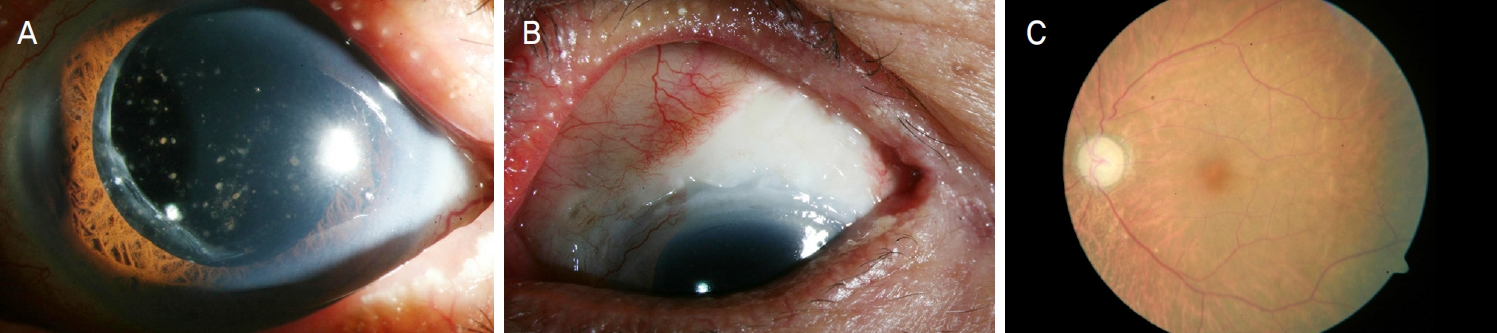
Anterior segment and fundus photographs 6 months after vitrectomy. (A) Clear anterior segment including cornea was seen. (B) The flat, avascular bleb remained. (C) Fundus was observed clearly.
고 찰
XEN® Gel Stent는 돼지 피부의 젤라틴 성분으로 구성된 친수성의 스텐트로 길이는 6 mm, 내직경 45 μm의 크기를 가진다[2]. XEN® Gel Stent 삽입술은 스텐트가 미리 장착된 특수 삽입기구를 이용하여 각막윤부의 작은 절개창을 통해 전방에서부터 결막아래 공간으로 스텐트를 삽입하는 수술이다[2]. 결막아래 공간으로 유출된 방수는 여과포를 형성하게 되며 여과포가 형성될 결막아래 공간에 마이토마이신C 주입을 스텐트 삽입 전에 시행한다[2]. XEN® Gel Stent 삽입술은 단독으로 또는 백내장수술과 함께 시행되고 있으며, 수술 후 30%의 안압하강률과 94.6%의 사용 약제 수의 감소를 보였다[1]. 또한 XEN® Gel Stent 삽입술은 섬유주절제술과 비교하여 비슷한 수준의 성공률을 보이면서 보다 높은 안정성을 갖는 것으로 보고되었다[3].
일반적으로 녹내장수술 후 안내염 발생률은 0.061%에서 1.80% 사이로 보고되어 왔다[5]. 섬유주절제술 후 여과포 연관 안내염 발생률은 2% 미만으로 보고되었으며, 녹내장 방 수유출장치 삽입술 후 안내염 발생률은 0.7%로 보고되었다[6,7]. 하지만 XEN® Gel Stent 삽입술 후 발생한 안내염은 몇몇의 외국 증례보고들이 있으며 아직 국내보고는 없다. 따라서 XEN® Gel Stent 관련된 안내염의 발생 빈도나 임상 양상에 대해서는 자세히 알려진 바가 없다.
일반적으로 녹내장수술 후 형성된 여과포와 관련된 감염은 대개 국소적인 여과포 부위의 염증으로 시작하여 점차 심한 안내염으로 진행한다[8]. 초기 증상은 결막충혈, 분비물, 자극감, 통증, 시력저하로 나타나며 여과포의 화농성 침윤, 여과포 누출이 발생할 수도 있고, 후기에는 전방염증, 전방축농, 유리체염증이 나타난다[8]. XEN® Gel Stent 삽입술도 결막아래 공간으로 유출된 방수에 의해 여과포가 형성되기 때문에 여과포와 연관된 감염이 발생할 수 있다. 또한 이식된 XEN® Gel Stent가 결막으로 밀려 나오면서 스텐트의 노출에 따른 감염도 발생할 수 있다.
Kerr et al [9]은 XEN® Gel Stent 삽입술 후 지연성으로 발생한 여과포 연관 감염을 3예 보고하였는데, 2예는 안내염이었다. 안내염이 발생하였던 2예 중 1예는 백내장수술과 함께 XEN® Gel Stent 삽입술을 받은 후 7개월째 안내염이 발생하였으며, 안내염 발생 4개월 전 XEN® Gel Stent가 결막 밖으로 노출되어 있어 일부 절제하고 결막아래 공간으로 밀어 넣었던 병력이 있었다. 다른 1예는 XEN® Gel Stent 삽입술을 받은 후 2년째 안내염이 발생하였으며, 무혈관성의 여과포 위 결막상피의 결손이 동반되어 있었다. Olgun et al [10]도 XEN® Gel Stent 삽입술 후 발생한 안내염 2예를 보고하였는데, 첫 증례는 만성 눈꺼풀염으로 치료받았던 병력이 있는 환자에서 XEN® Gel Stent 삽입술을 받은 후 5개월째 안내염이 발생하였으며, XEN® Gel Stent 노출은 관찰되지 않았다. 두 번째 증례는 XEN® Gel Stent 삽입술을 받은 후 4개월째 안내염이 발생하였으며, 결막 밖으로 밀려 나와있는 XEN® Gel Stent가 관찰되었다. Karri et al [11]은 술 후 4개월째에 발생한 XEN® Gel Stent 노출에 따른 안내염 1예를 보고하였다. 이전 보고들을 통해 XEN® Gel Stent 관련한 안내염 증례 5예 중 2예에서 XEN® Gel Stent 노출이 없이 발생하였음을 알 수 있었는데, 본 증례는 무혈관성 여과포에서 농의 누출은 있었으나 XEN® Gel Stent의 노출은 없었다. Olgun et al [10]와 Karri et al [11]은 이러한 증례들이 결막아래 주입된 mitomycin C가 결막상피와 기질의 위축을 유발해 XEN® Gel Stent 삽입술과 관련하여 여과포 연관된 안내염을 증가시킬 수 있다고 주장하였는데, 본 증례에서도 무혈관성 여과포의 위축된 결막파열과 이를 통한 안내염이 발생한 것으로 생각된다. 한편 지금까지 보고된 XEN® Gel Stent 관련 안내염들은 수술 후 4개월에서 2년째에 발생하였는데, 본 증례에서는 술 후 55일째 안내염이 발생하였으며, 이는 앞서 보고들에 비하여 비교적 빠른 시기에 발생한 것이었다.
본 증례에서 안내염의 원인균은 Streptococcus infantarius subsp. Infantarius였다. 이 균주는 Streptococcus bovis/equinus complex에 속하며, 사람과 동물의 담즙에서도 생존할 수 있는 소화기계의 상재균이다. 건강한 사람의 약 10%에서는 분변에서도 발견된다. Streptococcus bovis에 의한 안내염 보고는 있으나 Streptococcus infantarius에 의한 안내염 보고는 아직 없다. 일반적인 섬유주절제술 후 여과포 연관 안내염의 원인균은 수술 후 4주 이내에는 Coagulase negative Staphylococcus가 가장 흔하고 수술 후 4주 이후에는 Streptococcus species가 가장 흔한 것으로 알려져 있다[8]. Streptococci species는 백내장수술 후 안내염의 두 번째로 흔한 원인균이기도 하며, 외독소를 분비하고 여과포 위의 결막을 뚫고 들어갈 수 있어 눈 안으로 빠르게 퍼질 수 있다[12]. Streptococci species 안내염은 빠른 치료에도 불구하고 예후가 나쁜 것으로 알려져 있으며[13] 이전에 보고된 XEN® Gel Stent 관련 안내염의 원인균에는 Enterococcus faecalis, Moraxella nonliquefaciens 등이 있었다. Enterococcus faecalis는 구강 또는 소화기에 상재하는 그람양성균이며, 세균성 안내염의 원인균이 될 수 있으나 그 빈도는 아주 드물다[14]. Enterococcus faecalis 안내염은 진행이 빠르고 많은 항생제에 내성을 보여 예후가 불량한 것이 특징이다[14]. Moraxella nonliquefaciens는 상기도에 상재하는 그람음성균으로 발병력이 낮은 것으로 보인다[15]. Moraxella nonliquefaciens 안내염은 대개 지연성으로 여과포와 관련되어 발생하며 다른 지연성 여과포 관련 안내염과 다르게 대부분의 항생제에 감수성을 보여 예후가 좋다[15].
한편, XEN® Gel Stent 삽입술은 전방을 통한 안구 내 접근법(Ab interno)과 결막을 통한 안구 외 접근법(Ab externo)으로 시행될 수 있는데, 본 증례에서는 여과포의 화농성 농뒤로 봉합사가 관찰되어(Fig. 1D), 이를 수술 중에 제거하였다. 환자가 안구 외 접근법을 통하여 XEN® Gel Stent 삽입술을 시행받은 뒤 결막을 봉합한 것으로, 이렇게 남겨진 봉합사를 통해서도 감염이 발생하였을 수도 있었다고 생각된다.
저자들은 XEN® Gel Stent 삽입술 후 발생한 Streptococcus infantarius 안내염에서 XEN® Gel Stent 제거, 유리체절제술, 눈속 항생제 주입술을 시행하여 성공적으로 치료할 수 있었다. 본 증례를 통해 지금까지 보고된 증례들보다는 이른 시기에 XEN® Gel Stent 삽입술 관련 안내염이 발생한 것을 알 수 있었으며, 이를 조기에 진단하기 위해서는 수술 후 여과포에 대해 면밀한 검사가 권장된다. 또한 안내염이 의심될 때에는 XEN® Gel Stent의 빠른 수술적 제거와 적절한 눈속 항생제 치료가 필요하다.
Notes
This work supported by clinical research grant from Pusan National University Hospital in 2021.
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
김동선 / Dong Seon Kim
부산대학교 의과대학 안과학교실
Department of Ophthalmology, Pusan National University School of Medicine
