

ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØĆ Ļ░üļ¦ēņāüĒö╝ņØś ņĀäņĖĄ ņåīņŗżņØ┤ ļ░£ņāØĒĢ£ Ēøä, ņ×öņŚ¼ Ļ░üļ¦ēņāüĒö╝ņäĖĒż ļśÉļŖö Ļ░üļ¦ēņ£żļČĆņżäĻĖ░ņäĖĒżņŚÉ ņØśĒĢśņŚ¼ Ļ░üļ¦ēņØś ņ×¼ņāüĒö╝ĒÖöĻ░Ć ņØ╝ņ¢┤ļéśņ¦Ć ņĢŖņĢä ņĀĢņāüņĀüņØĖ ĻĄ¼ņĪ░ļź╝ ņ£Āņ¦ĆĒĢĀ ņłś ņŚåņØä ļĢī ļéśĒāĆļé£ļŗż. Ļ░üļ¦ēņØś ņ×¼ņāüĒö╝ĒÖöļź╝ ņĀĆĒĢ┤ĒĢśļŖö ņøÉņØĖņ£╝ļĪ£ļŖö ļłłļ¼╝ ņåŹņØś ņä▒ņןņØĖņ×ÉņØś ļČĆņĪ▒, 5ļ▓ł ļćīņŗĀĻ▓ĮņØś 3ņ░© ņŗĀĻ▓ĮņŚÉņä£ ļČäļ╣äļÉśļŖö neuropeptideņØś ļČĆņĪ▒ ĻĘĖļ”¼Ļ│Ā cytokineņØś ļČĆņĪ▒ ļō▒ņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1]. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØĆ Ļ░üļ¦ēņ░░Ļ│╝ņāüĻ│╝ ņłśņłĀ ļō▒ Ļ░üļ¦ēņŚÉ ļ░£ņāØĒĢśļŖö ņÖĖņāü, ņĢłĻĄ¼Ļ▒┤ņĪ░ņ”Ø, ļģĖņČ£Ļ░üļ¦ēņŚ╝, ņŗĀĻ▓Įņśüņ¢æĻ░üļ¦ēņŚ╝, Ļ░ÉņŚ╝Ļ░üļ¦ēņŚ╝ ņØ┤ĒøäņŚÉ ļ░£ņāØĒĢ£ Ļ░üļ¦ēĻČżņ¢æ ĻĘĖļ”¼Ļ│Ā ļŗ╣ļć©ņÖĆ Ļ░ÖņØĆ ņĀäņŗĀņ¦łĒÖś ļō▒ņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗż[2]. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØĆ ĒöīļŻ©ņśżļĀłņŗĀ ņŚ╝ņāēņ£╝ļĪ£ Ļ▓░ņåÉ ļČĆļČäņØ┤ ņŚ╝ņāēļÉśĻ│Ā ņŻ╝ļ│Ćņ£╝ļĪ£ Ļ░äņ£Āļ”¼ ļ¬©ņ¢æņØś Ēś╝ĒāüņØ┤ ļéśĒāĆļéśļ®░ ņŗ£ļĀźņĀĆĒĢśļź╝ ņ£Āļ░£ĒĢ£ļŗż. ļ¦īņĢĮ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØ┤ ņĀüņĀłĒĢ£ ņ╣śļŻīļź╝ ļ░øņ¦Ć ļ¬╗ĒĢ£ļŗżļ®┤, ņØ┤ņ░© Ļ░ÉņŚ╝, ļ░śĒØöĒśĢņä▒ ĻĘĖļ”¼Ļ│Ā ņ▓£Ļ│Ą ļō▒ņØś ĒĢ®ļ│æņ”ØņØ┤ ļ░£ņāØĒĢśņŚ¼ ņśüĻĄ¼ņĀüņØĖ ņŗ£Ļ░üņןņĢĀļź╝ ņØ╝ņ£╝Ēé¼ ņłś ņ׳ļŗż[3]. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņŚÉņä£ ļŗżņ¢æĒĢ£ ļ╣äņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓ĢĻ│╝ ņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓ĢņØ┤ ņŗ£Ē¢ēļÉśĻ│Ā ņ׳ņ£╝ļ®░, ĻĖ░ņĪ┤ņØś ļ╣äņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ļŖö ņØĖĻ│Ąļłłļ¼╝, Ļ│Āņןņä▒ ņĢłņĢĮ, Ēśłņ▓ŁņĢłņĢĮ ĻĘĖļ”¼Ļ│Ā ņ╣śļŻīņÜ® ņĮśĒāØĒŖĖļĀīņ”ł ļō▒ņØ┤ ņ׳ļŗż[4-8]. ņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ļŖö ņŻĮņØĆņĪ░ņ¦üņĀ£Ļ▒░ņłĀ ĻĘĖļ”¼Ļ│Ā ņ¢æļ¦ēņØ┤ņŗØņłĀņØ┤ ņŗ£Ē¢ēļÉśĻ│Ā ņ׳ļŗż[9-11]. ņ£äņÖĆ Ļ░ÖņØĆ ļŗżņ¢æĒĢ£ ņ╣śļŻī ļ░®ļ▓ĢņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ĒśĖņĀäņØä ļ│┤ņØ┤ņ¦Ć ņĢŖļŖö ļé£ņ╣śņä▒ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØĆ ņŗ£ļĀźņĀĆĒĢś ļ░Å ņéČņØś ņ¦łņØś ņĀĆĒĢśļź╝ ņØ╝ņ£╝Ēé©ļŗż.
ņ¢æļ¦ēņØĆ Ēā£ņĢäļ¦ē ņżæ Ļ░Ćņן ņĢłņ¬ĮņŚÉ ņ׳ļŖö ļ¦ēņ£╝ļĪ£, ņןļ▓Į ņŚŁĒĢĀņØä ĒĢśļŖö ļæÉĻ║╝ņÜ┤ ņĮ£ļØ╝Ļ▓ÉņĖĄĻ│╝ 4ĒśĢ ņĮ£ļØ╝Ļ▓É ļ░Å ļØ╝ļ»ĖļŗīņØä ĒżĒĢ©ĒĢ£ ĻĖ░ņĀĆļ¦ē ņä▒ļČäņ£╝ļĪ£ ĻĄ¼ņä▒ļÉśņ¢┤ ņ׳ņ£╝ļ®░, ņØ┤ņŗØņØä ĒĢśņŚ¼ļÅä Ļ▒░ļČĆļ░śņØæņØ┤ ņŚåļŗżļŖö ĒŖ╣ņ¦ĢņØä Ļ░Ćņ¦äļŗż[12]. ĻĘĖļ”¼Ļ│Ā ņ¢æļ¦ēņØĆ ņāüĒö╝ņäĖĒżņØś ņØ┤ļÅÖĻ│╝ ņ”ØņŗØ, ļČäĒÖöļź╝ ņ┤ēņ¦äĒĢśĻ│Ā ĻĖ░ņĀĆņāüĒö╝ņäĖĒżņØś ļČĆņ░®ņØä ņÜ®ņØ┤ĒĢśĻ▓ī ĒĢśļ®░, Ļ░üņóģ ņä▒ņןņØĖņ×É ļ░Å ļŗ©ļ░▒ņ¦ł ļČäĒĢ┤ņ¢ĄņĀ£ĒÜ©ņåīļź╝ ĒĢ©ņ£ĀĒĢśĻ│Ā ņ׳ņ¢┤, Ļ░üļ¦ēĒæ£ļ®┤ņ¦łĒÖśņŚÉņä£ ļ░£ņāØĒĢśļŖö ņäĖĒżņØś ņŻĮņØīņØ┤ļéś Ļ│Āņé¼ļź╝ ņ¢ĄņĀ£ĒĢśļŖö ĒŖ╣ņ¦ĢņØä Ļ░Ćņ¦äļŗż[13]. ņ¢æļ¦ēņØś ņØ┤ļ¤¼ĒĢ£ ĒŖ╣ņä▒ņØä ņØ┤ņÜ®ĒĢ£ ņ¢æļ¦ēņØ┤ņŗØņłĀņØĆ ņŻ╝ļĪ£ ļ┤ēĒĢ®ņé¼ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņ¢æļ¦ēņØä Ļ░üļ¦ēņŚÉ ņ£Āņ░®ņŗ£ĒéżļŖöļŹ░, ĒÖöņāüņŚÉ ņØśĒĢ£ Ļ░üļ¦ēņåÉņāü, ņŖżĒŗ░ļĖÉņŖż-ņĪ┤ņŖ©ņ”ØĒøäĻĄ░, ņĢłĻĄ¼ ņ£Āņé¼ņ▓£Ēżņ░Į ļō▒ ņŗ¼ĒĢśĻ▓ī ņåÉņāüļÉ£ ņĢłĻĄ¼Ēæ£ļ®┤ņ¦łĒÖśņØś ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ņä£ Ēśäņ×¼ ņ×äņāüņĀüņ£╝ļĪ£ ļäÉļ”¼ ņō░ņØ┤Ļ│Ā ņ׳ļŗż. Tseng [14]ņØĆ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņŚÉņä£ ņ¢æļ¦ēņØ┤ņŗØņłĀņØĆ ļ╣ĀļźĖ Ļ░üļ¦ēņāüĒö╝ĒÜīļ│Ą ļ░Å ņĢłĻĄ¼Ēæ£ļ®┤ņŚ╝ņ”ØņØä Ļ░Éņåīņŗ£ņ╝£ ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ ļ│┤Ļ│ĀĒĢśņśĆļŗż[15-18].
ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ņ¢æļ¦ēņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¦īļōĀ ņĀÉņĢłņĢĪņ£╝ļĪ£ ņ¢æļ¦ēĻ│╝ Ļ░ÖņØ┤ ņŚ╝ņ”Ø, ĒśłĻ┤Ć ņāØņä▒, ļ░śĒØöĒśĢņä▒ņØä ņ¢ĄņĀ£ĒĢśļŖö ļ¦ÄņØĆ ņä▒ņןņØĖņ×ÉņØś ļåŹļÅäĻ░Ć ļåÆņĢä Ļ░üļ¦ēņāüĒö╝ņåÉņāüņØś ĒÜīļ│ĄņØä ņ┤ēņ¦äĒĢśļŖö ĒŖ╣ņ¦ĢņØä Ļ░Ćņ¦äļŗż[13,19,20]. Liang et al [21]Ļ│╝ Sheha et al [22]ņØĆ ĻĖēņä▒ Ļ░üļ¦ēĒÖöņāüņ£╝ļĪ£ ņØĖĒĢ£ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×ÉņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņ╣śļŻīļĪ£ ņĢłĻĄ¼ņŚ╝ņ”ØņØä ņżäņØ┤Ļ│Ā ņ×¼ņāüĒö╝ĒÖöļź╝ ņ┤ēņ¦äĒĢśņśĆļŗżĻ│Ā ļ░£Ēæ£ĒĢśņśĆļŗż. ņØ┤ņŚÉ ļ│Ė ņŚ░ĻĄ¼ļŖö ĻĖ░ņĪ┤ņØś ņ╣śļŻīņŚÉ ĒśĖņĀäņØä ļ│┤ņØ┤ņ¦Ć ņĢŖļŖö ļé£ņ╣śņä▒ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×ÉņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØś ņ×äņāüņĀü ĒÜ©Ļ│╝ņŚÉ ļīĆĒĢśņŚ¼ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢśņśĆļŗż.
ļīĆņāüĻ│╝ ļ░®ļ▓Ģ
ļ│Ė ņŚ░ĻĄ¼ļŖö 2019ļģä 3ņøöļČĆĒä░ 2020ļģä 3ņøöĻ╣īņ¦Ć ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņ£╝ļĪ£ ņ¦äļŗ©ļ░øĻ│Ā ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØä ņé¼ņÜ®ĒĢ£ ņä▒ņØĖ ĒÖśņ×É 16ļ¬ģ 16ņĢłņØś ņØśļ¼┤ĻĖ░ļĪØņØä ĒøäĒ¢źņĀüņ£╝ļĪ£ ļČäņäØĒĢśņśĆļŗż. ņ¢æļ¦ē ņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņé¼ņÜ® ņĀä ņČ®ļČäĒĢ£ ņäżļ¬ģ ļ░Å ļÅÖņØśņä£ļź╝ ņ×æņä▒ Ēøä ņ╣śļŻīļź╝ ņŗ£ņ×æĒĢśņśĆņ£╝ļ®░, ĒŚ¼ņŗ▒ĒéżņäĀņ¢ĖņØä ņżĆņłśĒĢśĻ│Ā Institutional Review Board (IRB) ņ£äņøÉĒÜīņØś ņŖ╣ņØĖņØä ļ░øņĢäņä£ ņŚ░ĻĄ¼ļź╝ ņ¦äĒ¢ēĒĢśņśĆļŗż(ņŖ╣ņØĖ ļ▓łĒśĖ: CNUH-2021-140).
ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØĆ ņØĖĻ│Ąļłłļ¼╝, ĒĢŁņāØņĀ£ņĢłņĢĮ, ņ╣śļŻīņÜ® ņĮśĒāØĒŖĖļĀīņ”łņÖĆ Ļ░ÖņØĆ ĻĖ░ņĪ┤ ļ╣äņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ ņ╣śļŻīĒĢśņŚ¼ļÅä 4ņŻ╝ ņØ┤ņāü ļÅÖņĢł ĒśĖņĀäņØ┤ ņŚåĻ│Ā Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś ļ®┤ņĀüņØ┤ ņĄ£ņåī 2 mm2 ņØ┤ņāüņØĖ Ļ▓ĮņÜ░ļĪ£ ņĀĢņØśĒĢśņśĆņ£╝ļ®░, ņ╣©ņŖĄņĀü ņŗ£ņłĀ ļśÉļŖö ņłśņłĀņĀü ņ╣śļŻīļź╝ ņŗ£Ē¢ē ļ░øĻ▒░ļéś, ņ×ÉņØśņĀüņ£╝ļĪ£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņé¼ņÜ®ņØä ņżæļŗ©ĒĢ£ Ļ▓ĮņÜ░, 2Ļ░£ņøö ņØ┤ņāü Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØä ĒĢśņ¦Ć ļ¬╗ĒĢ£ Ļ▓ĮņÜ░ļŖö ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņĀ£ņÖĖļÉśņŚłļŗż. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×ÉļōżņØĆ ĻĖ░ņĪ┤ ņ╣śļŻīļĪ£ ļ¼┤ļ░®ļČĆņĀ£ 0.15% Ē׳ņĢīļŻ©ļĪĀņé░ ļéśĒŖĖļź©(Hyaluni eye drops 0.15%┬«, Taejoon Pharmaceutical Co., Ltd., Seoul, Korea) ĒĢśļŻ©ņŚÉ 6ĒÜī ņØ┤ņāü, 0.5% ļĀłļ│┤ĒöīļĪØņé¼ņŗĀ(Cravit┬«, Santen Pharmaceutical Co., Ltd., Osaka, Japan) ĒĢśļŻ©ņŚÉ 2-4ĒÜī, ĻĘĖļ”¼Ļ│Ā ņ£żĒÖ£ņÜ® ņŚ░Ļ│Ā(Duratears┬«, Alcon Laboratories, Inc., Fort Worth, TX, USA)ļź╝ ņĘ©ņ╣© ņĀä ĒĢ£ļ▓ł ļÅäĒżĒĢśņśĆĻ│Ā, ņĢłĻĄ¼ Ēæ£ļ®┤ņŚÉ ņŚ╝ņ”ØņØ┤ ņ׳ļŗżļ®┤ 5% ļĪ£ĒģīĒöäļĀłļō£ļåĆ(Lotemax┬«, Bausch & Lomb, New York, NY, USA)ņØä ĒĢśļŻ© 2-3ĒÜī 1ņŻ╝Ļ░ä ņĀÉņĢłĒĢśņśĆļŗż. ņ╣śļŻīņŚÉļÅä 4ņŻ╝ ņØ┤ņāü Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś ĒśĖņĀäņØ┤ ņŚåļŖö Ļ▓ĮņÜ░ ĻĖ░ņĪ┤ ņĢłņĢĮņŚÉ ļŹöĒĢśņŚ¼ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØä ĒĢśļŻ© 6ĒÜī ņĀÉņĢłĒĢśņśĆļŗż.
ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ļČäļ”¼ļÉ£ ņØĖĻ░ä ņ¢æļ¦ēņØä ĒÄśļŗłņŗżļ”░Ļ│╝ ņŖżĒŖĖļĀÖĒåĀļ¦łņØ┤ņŗĀņØä ĒżĒĢ©ĒĢ£ ņāØļ”¼ņŗØņŚ╝ņłśļĪ£ ņäĖņ▓Ö Ēøä ļ®öņŖżļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņ×æņØĆ ņĪ░Ļ░üļōżļĪ£ ņלļØ╝ ņĢĪņ▓┤ ņ¦łņåīņŚÉ ļäŻņ¢┤ ļÅÖĻ▓░ Ļ▒┤ņĪ░ĒĢ£ Ēøä ļČäņćäĒĢśņŚ¼ ļ¼┤Ļ▓ī(g)ļź╝ ņĖĪņĀĢĒĢśņŚ¼ 2ļ░░ņØś ļČĆĒö╝(mL)ņØś ņ”ØļźśņłśņÖĆ Ēś╝ĒĢ®ĒĢ£ ļÆż ņ┤łņØīĒīī ļČäņćäĻĖ░(UP200S-Heilescher, Teltow, Germany)ļĪ£ ĻĘĀņ¦łĒÖöņŗ£ņ╝░Ļ│Ā, ĻĘĖ Ēøä ņøÉņŗ¼ļČäļ”¼(4Ōäā 4,000 gņŚÉņä£ 10ļČäĻ░ä)ļź╝ ņŗ£Ē¢ēĒĢśņŚ¼ ņāüņĖĄņĢĪņØä ņłśņ¦æĒĢ£ ļÆż ņāüņĖĄņĢĪņØä ļŗżņŗ£ ņøÉņŗ¼ļČäļ”¼(4Ōäā 15,000 gņŚÉņä£ 5ļČäĻ░ä)ļź╝ ĒĢ£ Ēøä 0.25 ╬╝m ĒĢäĒä░(MILLEX GS, Millipore, Billerica, MA, USA)ļź╝ ĒåĄĻ│╝ņŗ£ņ╝£ ļ®ĖĻĘĀĒĢśņŚ¼ ņĀ£ņĪ░ĒĢśņśĆļŗż[13]. ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØä 2ņŻ╝ļ¦łļŗż ņĀ£ņĪ░ĒĢśņŚ¼ ņĀ£Ļ│ĄĒĢśņśĆĻ│Ā, ĒÖśņ×ÉļōżņŚÉĻ▓ī ļāēņן ļ│┤Ļ┤ĆĒĢśļÅäļĪØ ņ¦Ćņŗ£ĒĢśņśĆļŗż.
ļéśņØ┤, ņä▒ļ│ä ĻĘĖļ”¼Ļ│Ā Ļ│╝Ļ▒░ļĀźĻ│╝ Ļ░ÖņØĆ ĒÖśņ×ÉļōżņØś ĒŖ╣ņ¦Ģ, ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØä ņ£Āļ░£ĒĢ£ ņĢłĻ│╝ņĀü ņ¦łĒÖś ĻĘĖļ”¼Ļ│Ā ņ▓śņØī ņ¦äļŗ© ņŗ£ļČĆĒä░ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņé¼ņÜ®Ļ╣īņ¦Ć Ļ▒Ėļ”░ ĻĖ░Ļ░äņŚÉ ļīĆĒĢśņŚ¼ ņĪ░ņé¼ĒĢśņśĆļŗż. ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņ╣śļŻī ņĀä, ņ╣śļŻī Ēøä 1Ļ░£ņøöņ¦Ė, 2Ļ░£ņøöņ¦Ė ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀź, ņĢłĻĄ¼ĒåĄņ”ØņĀÉņłś, Ļ░üļ¦ēņ¦ĆĻ░üņĀÉņłś, Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ®┤ņĀüņØä ņĖĪņĀĢĒĢśņśĆļŗż. ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀźņØĆ logarithm of minimal angle of resolution (LogMAR)ļĪ£ ļ│ĆĒÖśĒĢśņśĆĻ│Ā, ņĢłĻĄ¼ĒåĄņ”ØņĀÉņłśļŖö visual analogue scale ņĀÉņłś(0-10ņĀÉ. 0ņĀÉ: ĒåĄņ”Ø ņŚåņØī, 10ņĀÉ: ņĢäņŻ╝ ņŗ¼ĒĢ£ ņ░ĖņØä ņłś ņŚåļŖö ņĄ£Ļ│ĀņØś ĒåĄņ”Ø)ļĪ£ ņłśņ╣śĒÖöĒĢśņśĆļŗż. Ļ░üļ¦ēņ¦ĆĻ░üņĀÉņłś(esthesiometer)ļŖö Ļ░üļ¦ēņ¦ĆĻ░üĻ│ä(Cochet-Bonnet esthesiometer┬«, Luneau Ophthalmology, Chartres Cedex, France)ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ļéśņØ╝ļĪĀ ņäĖņé¼ļź╝ ņĄ£ļīĆĒĢ£ņ£╝ļĪ£ ļŖśļ”░ Ēøä ĻĘĖ ļüØņØä Ļ░üļ¦ē ņżæņŗ¼ļČĆņŚÉ ņłśņ¦üņ£╝ļĪ£ ņĀæņ┤ēņŗ£Ēéżļ®░ ņäĖņé¼ņØś ĻĖĖņØ┤ļź╝ ļŗ©Ļ│äņĀüņ£╝ļĪ£ ņżäņŚ¼Ļ░Ćļ®┤ņä£ Ēö╝Ļ▓Ćņ×ÉĻ░Ć ņ▓śņØīņ£╝ļĪ£ Ļ░ÉĻ░üņØä ļŖÉļéä ļĢīņØś ņäĖņé¼ņØś ĻĖĖņØ┤ļź╝ 3ĒÜī ļ░śļ│Ą ņĖĪņĀĢ Ēøä ĒÅēĻĘĀĻ░ÆņØä ļ░Ćļ”¼ļ»ĖĒä░ļĪ£ ņĖĪņĀĢĒĢśņśĆļŗż. Ļ░üļ¦ēņāüĒö╝ņäĖĒżĻ▓░ņåÉņØś ļ®┤ņĀüņØĆ 1% fluorescein ņŚ╝ņāēņĢĪ 2 ╬╝Lļź╝ ļ¦łņØ┤Ēü¼ļĪ£Ēö╝ĒĽņ£╝ļĪ£ Ļ▓░ļ¦ēļéŁņŚÉ ņĀÉņĀüĒĢ£ ļÆż ņĀäņĢłļČĆ ņé¼ņ¦äņØä ņäĖĻĘ╣ļō▒Ēśäļ»ĖĻ▓Į(Haag-Streit BQ900, Hagg-Streit AG, K├Čniz, Switzerland)ņŚÉ ļČĆņ░®ļÉ£ 10ļ░░ņ£©ņØś ņ╣┤ļ®öļØ╝(DC4, Topcon, Tokyo, Japan)ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņ┤¼ņśüĒĢ£ Ēøä ņןņČĢņØś ĻĖĖņØ┤ņÖĆ ļŗ©ņČĢņØś ĻĖĖņØ┤ļź╝ Ļ│▒ĒĢśņŚ¼ņä£ ņĖĪņĀĢĒĢśņśĆļŗż[23]. ņ╣śļŻī Ļ▓░Ļ│╝ļŖö ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņé¼ņÜ® 2Ļ░£ņøöņ¦Ė ņāüĒö╝Ļ▓░ņåÉņØ┤ ņÖäņĀäĒ׳ ĒÜīļ│ĄļÉśļ®┤ ĒÜ©Ļ│╝ņĀü, ņé¼ņÜ® ņĀäĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś ļ®┤ņĀüņØ┤ Ļ░ÉņåīĒĢśņśĆņ£╝ļéś ļé©ņĢäņ׳ļŖö Ļ▓ĮņÜ░ ļČĆļČä ĒÜ©Ļ│╝ņĀü, Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś ļ®┤ņĀüņØś ļ│ĆĒÖöĻ░Ć ņŚåņ¢┤ ņČöĻ░ĆņĀüņØĖ ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢ£ Ļ▓ĮņÜ░ ĒÜ©Ļ│╝ ņŚåņØīņ£╝ļĪ£ ĒīÉņĀĢĒĢśņśĆļŗż.
ĒåĄĻ│äņĀü ļČäņäØņØĆ SPSS Statistics for Windows, version 18.0 (IBM Corp., Armonk, NY, USA)ļź╝ ņØ┤ņÜ®ĒĢśņśĆĻ│Ā ņłśņ╣śļŖö ĒÅēĻĘĀ ┬▒ Ēæ£ņżĆĒÄĖņ░©ļĪ£ ļéśĒāĆļāłļŗż. Wilcoxon signed-rank testļŖö ņ╣śļŻī ņĀäĒøä ļ│ĆĒÖöļź╝ ļ╣äĻĄÉĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ņé¼ņÜ®ĒĢśņśĆĻ│Ā, p-valueĻ░Ć 0.05ļ│┤ļŗż ņ×æņØĆ Ļ▓ĮņÜ░ ĒåĄĻ│äņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśļŗżĻ│Ā Ļ░ĆņĀĢĒĢśņśĆļŗż.
Ļ▓░ Ļ│╝
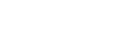
ĻĖ░ņĪ┤ ņ╣śļŻīņŚÉ ļ░śņØæĒĢśņ¦Ć ņĢŖņØĆ ļé£ņ╣śņä▒ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×É 16ļ¬ģ 16ņĢłņØ┤ ņŚ░ĻĄ¼ņŚÉ ņ░ĖņŚ¼ĒĢśņśĆļŗż. ņ░ĖņŚ¼ĒĢ£ ĒÖśņ×ÉļōżņØś ļéśņØ┤ļŖö 67.50 ┬▒ 12.41ņäĖņśĆņ£╝ļ®░, ļé©ņä▒ņØ┤ 9ļ¬ģ(56.3%), ņŚ¼ņä▒ņØ┤ 7ļ¬ģ(43.8%)ņØ┤ņŚłļŗż. ļ¬©ļōĀ ĒÖśņ×ÉņŚÉņä£ ļŗ©ņĢłņŚÉ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØä ļ│┤ņśĆņ£╝ļ®░, 9ņĢł(56.3%)ņØĆ ņÜ░ņĢł, 7ņĢł(43.8%)ņØĆ ņóīņĢłņØ┤ņŚłļŗż. ĒÖśņ×ÉļōżņØś ņĀäņŗĀņ¦łĒÖśņ£╝ļĪ£ 10ļ¬ģ(62.5%)ņŚÉņä£ Ļ│ĀĒśłņĢĢ, 6ļ¬ģ(37.5%)ņŚÉņä£ ļŗ╣ļć©Ļ░Ć ņ׳ņŚłļŗż. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØä ņ£Āļ░£ĒĢ£ ņ¦łĒÖśņØĆ ĒŚżļź┤ĒÄśņŖżĻ░üļ¦ēņŚ╝ 6ņĢł(37.5%), ņŗĀĻ▓Įņśüņ¢æĻ░üļ¦ēņŚ╝ 8ņĢł(50.0%), ņĢłĻĄ¼ņØ┤ņŗØĒÄĖļīĆņłÖņŻ╝ļ│æ 1ņĢł(6.3%), Ļ░üļ¦ēņ£żļČĆņäĖĒżĻ▓░ĒĢŹņ”Ø 1ņĢł(6.3%)ņØ┤ņŚłļŗż. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņ£╝ļĪ£ ņ¦äļŗ©ļÉśĻ│Ā 120.2 ┬▒ 96.6ņØ╝ ĒøäņŚÉ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņé¼ņÜ®ņØä ņŗ£ņ×æĒĢśņśĆņ£╝ļ®░, ņ¦äļŗ© ņŗ£ ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀźņØĆ 0.8 ┬▒ 0.5 LogMAR, ņĢłĻĄ¼ĒåĄņ”ØņĀÉņłśļŖö 4.3 ┬▒ 1.0ņĀÉ, Ļ░üļ¦ēņ¦ĆĻ░üņĀÉņłśļŖö 7.6 ┬▒ 3.1 mm, Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ®┤ņĀüņØĆ 5.2 ┬▒ 3.1 mm2ņśĆļŗż(Table 1).
ņ¦ĆņåŹņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×ÉņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņ╣śļŻī ņĀäĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņ╣śļŻī Ēøä ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀźņØĆ 1Ļ░£ņøöņ¦Ė 0.7 ┬▒ 0.3 LogMAR (p=0.04), 2Ļ░£ņøöņ¦Ė 0.6 ┬▒ 0.3 LogMAR (p=0.03)ļĪ£ ņ”ØĻ░ĆĒĢśņśĆļŗż(Fig. 1A). ņĢłĻĄ¼ĒåĄņ”ØņĀÉņłśļŖö 1Ļ░£ņøöņ¦Ė 4.0 ┬▒ 0.8ņĀÉ(p=0.10)ņ£╝ļĪ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļéś, 2Ļ░£ņøöņ¦Ė 2.8 ┬▒ 0.7ņĀÉ(p=0.04)ņ£╝ļĪ£ Ļ░ÉņåīĒĢśņśĆļŗż(Fig. 1B). Ļ░üļ¦ēņ¦ĆĻ░üņĀÉņłśļŖö 1Ļ░£ņøöņ¦Ė 8.0 ┬▒ 3.5 mm (p=0.12), 2Ļ░£ņøöņ¦Ė 9.8 ┬▒ 3.6 mm (p=0.08)ļĪ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż(Fig. 1C). Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉļ®┤ņĀüņØĆ 1Ļ░£ņøöņ¦Ė 1.16 ┬▒ 1.1 mm2 (p=0.03), 2Ļ░£ņøöņ¦Ė 0.1 ┬▒ 0.1 mm2 (p=0.01)ļĪ£ Ļ░ÉņåīĒĢśņśĆļŗż(Fig. 1D).
ņ¢æļ¦ēņČöņČ£ļ¼╝ņĢłņĢĮņØĆ 13ņĢł(81.3%)ņŚÉņä£ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØ┤ ĒśĖņĀäļÉśņ¢┤ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłņ£╝ļ®░, ĒÅēĻĘĀ ņ╣śļŻī ĻĖ░Ļ░äņØĆ 2.92 ┬▒ 1.81ņŻ╝ņśĆļŗż. ļ░śļ®┤ 3ņĢł(18.8%)ņŚÉņä£ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ®┤ņĀü ļ░Å Ļ░üļ¦ēļČĆņóģņØĆ Ļ░ÉņåīĒĢśņśĆņ£╝ļéś, Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ░Å Ļ░üļ¦ēļČĆņóģņØ┤ ļé©ņĢäņ׳ņ¢┤ ļČĆļČä ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż(Table 2).
ļ¬©ļōĀ ĒÖśņ×ÉņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņé¼ņÜ® ņŗ£ ņČ®Ēśł, ļö░Ļ░ĆņøĆ ļō▒ņØś ļČĆņ×æņÜ®ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░ ņ×ÉņØśņĀüņ£╝ļĪ£ ņĀÉņĢłņØä ņżæļŗ©ĒĢśņ¦Ć ņĢŖņĢśļŗż. ņ╣śļŻī ĻĖ░Ļ░ä ņżæ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ®┤ņĀüņØ┤ ņ”ØĻ░ĆĒĢśņŚ¼ ņ¢æļ¦ēņØ┤ņŗØņłĀ ļō▒ņØś ņłśņłĀņĀü ņ▓śņ╣śļŖö ņŗ£Ē¢ēļÉśņ¦Ć ņĢŖņĢśņ£╝ļéś, ļČĆļČä ĒÜ©Ļ│╝ļź╝ ļ│┤ņØĖ ĒÖśņ×ÉļōżņØĆ ņØ┤Ēøä ņ¢æļ¦ēņØ┤ņŗØņłĀņØä ņŗ£Ē¢ēļ░øņĢśļŗż.
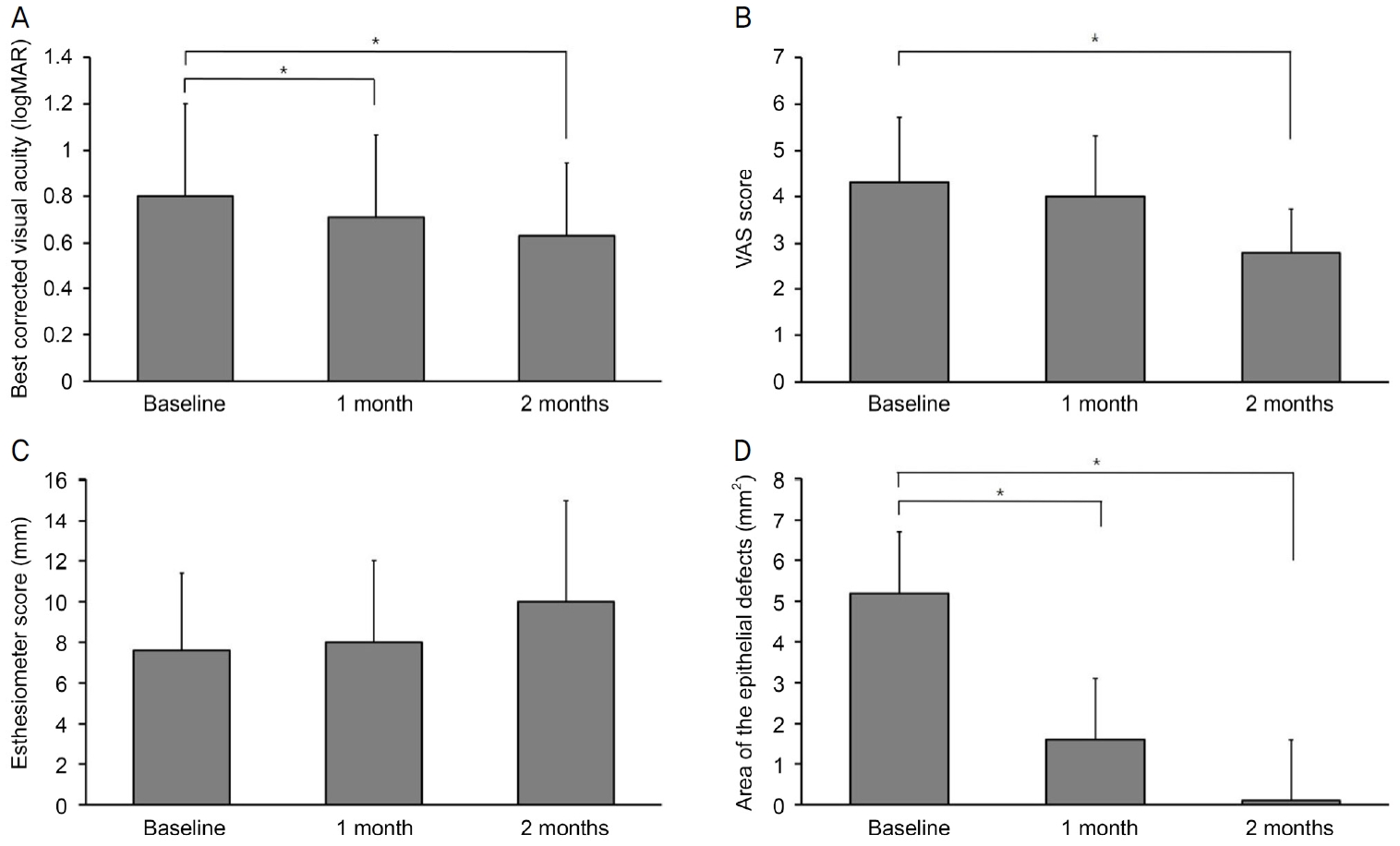
ņ”ØļĪĆ(ĒÖśņ×É ļ▓łĒśĖ 7)
41ņäĖ ņŚ¼ņä▒ņØĆ ļŗ╣ļć©ļ│æņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ£╝ļ®░ ņÜ░ņĢłņØś ņŗĀĻ▓Įņśüņ¢æĻ░üļ¦ēņŚ╝Ļ│╝ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØä ļ│┤ņśĆļŗż. ņÜ░ņĢłņØś ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉĻ│╝ ļÅÖļ░śļÉ£ ņŻ╝ļ│ĆļČĆ ņŗĀņāØĒśłĻ┤Ć ņåīĻ▓¼ņØ┤ ņ׳ņŚłĻ│Ā, ļ░śļīĆņĢłņØĆ ĒŖ╣ņØ┤ ņåīĻ▓¼ņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņ£╝ļĪ£ ņ¦äļŗ© ņŗ£ ĒÖśņ×ÉņØś ņŗ£ļĀźņØĆ 0.4 logMAR, Ļ░üļ¦ēņ¦ĆĻ░üņĀÉņłśļŖö 5 mmļĪ£ Ļ░ÉņåīļÉśņ¢┤ ņ׳ņ£╝ļ®░ ņÜ░ņĢłņØś ņŗ£ļĀźņĀĆĒĢśĻ░ÉĻ│╝ ĒåĄņ”Ø, ļłłļČĆņŗ¼, ļłłļ¼╝ ĒØśļ”╝ ņ”ØņāüņØä ĒśĖņåīĒĢśņśĆļŗż. 0.5% ļĀłļ│┤ĒöīļĪØņé¼ņŗĀ, ļ¼┤ļ░®ļČĆņĀ£ 0.15% Ē׳ņĢīļŻ©ļĪĀņé░ ļéśĒŖĖļź©, ņ£żĒÖ£ņÜ® ņŚ░Ļ│Ā ņé¼ņÜ®ĒĢśņŚ¼ ņ╣śļŻīļź╝ ņŗ£ņ×æĒĢśņśĆĻ│Ā, 2Ļ░£ņøöĻ░äņØś ņ╣śļŻīņŚÉļÅä Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś Ēü¼ĻĖ░ļŖö 10.37 mm2ļź╝ ļ│┤ņØ┤ļ®░, ĒśĖņĀäņØ┤ ņŚåņŚłņ£╝ļ®░ Ļ░üļ¦ēļČĆņóģļÅä ĒĢ©Ļ╗ś Ļ┤Ćņ░░ļÉśņŚłļŗż. ļö░ļØ╝ņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØä ĒĢśļŻ© 6ĒÜī ņĀÉņĢłņØä ņŗ£ņ×æĒĢśņśĆļŗż. ņ╣śļŻī 2Ļ░£ņøöņ¦Ė Ļ░üļ¦ēļČĆņóģĻ│╝ ņŻ╝ļ│ĆļČĆ ņŗĀņāØĒśłĻ┤ĆņØĆ Ļ░ÉņåīĒĢśņśĆĻ│Ā, Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ®┤ņĀüņØĆ 1.0 mm2ļĪ£ Ļ░ÉņåīĒĢśņśĆņ£╝ļéś ņŚ¼ņĀäĒ׳ ļé©ņĢä ņ׳ņŚłļŗż. ņ╣śļŻī ĻĖ░Ļ░ä ļÅÖņĢł ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņŚÉ ļīĆĒĢ£ ļČĆņ×æņÜ®ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 2).
Ļ│Ā ņ░░
ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØĆ Ļ░üļ¦ē ņåÉņāüņØ┤Ēøä ņ×öņŚ¼ Ļ░üļ¦ēņāüĒö╝ņäĖĒż ļśÉļŖö Ļ░üļ¦ēņ£żļČĆņżäĻĖ░ņäĖĒżņŚÉ ņØśĒĢśņŚ¼ Ļ░üļ¦ēņØś ņ×¼ņāüĒö╝ĒÖöĻ░Ć ņØ╝ņ¢┤ļéśņ¦Ć ņĢŖņĢä ņĀĢņāüņĀüņØĖ Ļ░üļ¦ēņØś ĻĄ¼ņĪ░ļź╝ ņ£Āņ¦ĆĒĢĀ ņłś ņŚåļŖö ņ¦łĒÖśņ£╝ļĪ£ ļŗżņ¢æĒĢ£ ņ╣śļŻī ļ░®ļ▓ĢņØ┤ ņŚ░ĻĄ¼ļÉśņŚłļŗż. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņŚÉņä£ Tsubota et al [4]ņØĆ 16ņĢłņŚÉņä£ ņ×ÉĻ░ĆĒśłņ▓ŁņĢłņĢĮ ņé¼ņÜ® ņŗ£ ĒÖśņ×ÉņØś 62.5%ņŚÉņä£ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØ┤ 1ļŗ¼ ņØ┤ļé┤ņŚÉ ĒśĖņĀäļÉśņ¢┤ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗżĻ│Ā ļ░£Ēæ£ĒĢśņśĆņ£╝ļ®░, Yoon et al [24]ņØĆ 14ņĢłņŚÉņä£ ņĀ£ļīĆĒśłņ▓ŁņĢłņĢĮ ņé¼ņÜ® ņŗ£ ĒÖśņ×ÉņØś 42.9%ņŚÉņä£ 2ņŻ╝ ņØ┤ļé┤ņŚÉ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØ┤ ĒśĖņĀäļÉśņŚłņ£╝ļ®░, 42.9%ņŚÉņä£ 2-4ņŻ╝ ņé¼ņØ┤ņŚÉ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØ┤ ĒśĖņĀäļÉśņ¢┤ ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻīļ▓ĢņØ┤ļØ╝ ļ░£Ēæ£ĒĢśņśĆļŗż. Moon et al [25]ņØĆ 15ņĢłņŚÉņä£ Ēæ£Ēö╝ņä▒ņןņØĖņ×É ņŚ░Ļ│Ā ņé¼ņÜ® ņŗ£ ĒÖśņ×ÉņØś 80%ņŚÉņä£ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØ┤ 2ļŗ¼ ņØ┤ļé┤ņŚÉ ĒśĖņĀäļÉśņŚłļŗżĻ│Ā ļ░£Ēæ£ĒĢśņśĆļŗż. ņØ┤ņÖĆ Ļ░ÖņØ┤ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØä ņ╣śļŻīĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ļŗżņ¢æĒĢ£ ļ░®ļ▓ĢļōżņØ┤ ņŚ░ĻĄ¼ļÉśņŚłļŗż.
ņ¢æļ¦ēņØĆ ņĢłĻ│╝ņśüņŚŁņŚÉņä£ 1995ļģä Kim and Tseng [26]ņØ┤ ņ¢æļ¦ēņØś ĻĖ░ļŖźņØä ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć ņĢłĻ│╝ ņ¦łĒÖśņŚÉ ņ×äņāüņĀüņ£╝ļĪ£ ņĀüņÜ®ņŗ£ĒéżļŖö ņŚ░ĻĄ¼ļź╝ ĒĢ£ ņØ┤Ēøä ņÖĖņĢłļČĆ ņ¦łĒÖśņŚÉ ņ׳ņ¢┤ņä£ ļŗżņ¢æĒĢśĻ▓ī ņØæņÜ®ļÉśņŚłļŗż. ņ¢æļ¦ēņØĆ ņĀĢņāüņĀüņØĖ ņāüĒö╝ņäĖĒżņØś ĒŖ╣ņä▒ņØä ņ£Āņ¦Ćņŗ£ĒéżĻ│Ā ņāüĒö╝ņäĖĒż ņä▒ņןņØä ņ┤ēņ¦äĒĢśļ®░ ĒĢŁņŚ╝ņ”Øņ×æņÜ®, ņŗĀņāØĒśłĻ┤Ć ņ¢ĄņĀ£ ņ×æņÜ® ļ░Å ļ░śĒØö ĒśĢņä▒ ņ¢ĄņĀ£ ņ×æņÜ® ļō▒ņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ņ£╝ļ®░, Ļ░üļ¦ē ļ░Å Ļ▓░ļ¦ē ļ¬©ņäĖĒżņØś ņä▒ņןĻ│╝ ĻĘĖ ĒŖ╣ņä▒ņØä ņ£Āņ¦Ćņŗ£Ēé¼ ņłś ņ׳ļŖö ĻĖ░ņĀĆļ¦ēņ£╝ļĪ£ ņ×æņÜ®ĒĢśļ»ĆļĪ£, ņāüĒö╝ņØś ņØ┤ļÅÖņØä ņ┤ēņ¦äņŗ£ĒéżĻ│Ā ņāüĒö╝ ĻĖ░ņĀĆņĖĄņØś ņ£Āņ░®ņØä Ļ░ĢĒÖöĒĢśļ®░, ļČäĒÖöļź╝ ņ┤ēņ¦äņŗ£ņ╝£ ņ░Įņāüņ╣śņ£Ā ņŗ£ ņāüĒö╝ņ×¼ņāØņØä ņ┤ēņ¦äņŗ£Ēé©ļŗż[26-30]. ĒĢ£ĒÄĖ ņ¢æļ¦ēņØĆ ņŚ╝ņ”ØņäĖĒżņØś ĒØĪņ░® ļ░Å transforming growth factor ņŗĀĒśĖņ▓┤Ļ│äņØś ĒĢśĒ¢źņĪ░ņĀĢņØä ĒåĄĒĢśņŚ¼ ņä¼ņ£ĀņĢäņäĖĒżņØś ņ”ØņŗØ ļ░Å ĻĘ╝ņä¼ņ£ĀļĪ£ņØś ļČäĒÖöļź╝ ņ¢ĄņĀ£ĒĢ┤ ļ░śĒØöĒśĢņä▒ņØä ņ¢ĄņĀ£ĒĢĀ ņłś ņ׳ļŗż[29].
ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ņ¢æļ¦ēņØä ļÅÖĻ▓░Ļ▒┤ņĪ░ĒĢśņŚ¼ ņĀ£ņĪ░ĒĢ£ ņĢłņĢĮņ£╝ļĪ£ ņ¢æļ¦ēĻ│╝ Ļ░ÖņØ┤ ĒĢŁņŚ╝ņ”Øņ×æņÜ®, ņŗĀņāØĒśłĻ┤Ć ņ¢ĄņĀ£ ņ×æņÜ®, ļ░śĒØöĒśĢņä▒ ņ¢ĄņĀ£ ņ×æņÜ®ņØä ĒĢśļŖö ļ¦ÄņØĆ ņä▒ņןņØĖņ×ÉņØś ļåŹļÅäĻ░Ć ļåÆņĢä ņ¢æļ¦ēņØ┤ņŗØņłĀĻ│╝ ņ£Āņé¼ĒĢśĻ▓ī Ļ░üļ¦ēņåÉņāüņØä ĒÜīļ│Ąņŗ£Ēé©ļŗż[13,19,20]. Kordi─ć et al [31]ņØĆ ņŗĀĻ▓Įņśüņ¢æņä▒Ļ░üļ¦ēņŚ╝Ļ│╝ ļÅÖļ░śļÉ£ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×É 2ļ¬ģ 2ņĢłņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØä 1ņŗ£Ļ░ä Ļ░äĻ▓®ņ£╝ļĪ£ ņé¼ņÜ®ĒĢ£ ņ╣śļŻīņŚÉņä£ 2ņŻ╝ Ēøä ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś ņÖäņĀäĻ┤ĆĒĢ┤ļź╝ ļ│┤ņśĆļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆĻ│Ā, Liang et al [21]ņØĆ ņżæņ”ØļÅäņØś Ļ░üļ¦ēĒÖöĒĢÖĒÖöņāüņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ Ļ░üļ¦ēņØś ņŚ╝ņ”ØņØä Ļ░Éņåīņŗ£ĒéżĻ│Ā ņ×¼ņāüĒö╝ĒÖöļź╝ ņ┤ēņ¦äĒĢśņŚ¼ ņ╣śļŻīņŚÉ ļÅäņøĆņØä ņŻ╝ņŚłļŗżĻ│Ā ĒĢśņśĆļŗż[22].
ļ│Ė ņŚ░ĻĄ¼ļŖö ĻĖ░ņĪ┤ ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ ĒśĖņĀäļÉśņ¦Ć ņĢŖņØĆ ļé£ņ╣śņä▒ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×É 16ļ¬ģņØä ļīĆņāüņ£╝ļĪ£ ĻĖ░ņĪ┤ ņ╣śļŻīņŚÉ ņČöĻ░ĆĒĢśņŚ¼ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØä ĒĢśļŻ©ņŚÉ 6ĒÜī ņé¼ņÜ®ĒĢśņśĆļŗż. ņ╣śļŻī ņĀäņŚÉ ļ╣äĒĢśņŚ¼ ņ╣śļŻī 2Ļ░£ņøöņ¦Ė ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀź, Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ļ®┤ņĀü ĻĘĖļ”¼Ļ│Ā ņĢłĻĄ¼ĒåĄņ”ØņĀÉņłśņØś ņ£ĀņØśĒĢ£ ĒśĖņĀäņØä ļ│┤ņśĆņ£╝ļéś, Ļ░üļ¦ēņ¦ĆĻ░üņĀÉņłśļŖö ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż. ņØ┤ļŖö ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØ┤ Ļ░üļ¦ēņāüĒö╝ĒÜīļ│ĄņŚÉ ļÅäņøĆņØ┤ ļÉśņŚłļŗżļŖö Kordi─ć et al [31]ņØś ņŚ░ĻĄ¼ņÖĆ ņ£Āņé¼ĒĢ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆņ¦Ćļ¦ī, ņ¢æļ¦ēņØś ņŗĀĻ▓Įņä▒ņןņØĖņ×Éļź╝ ĒåĄĒĢśņŚ¼ ņåÉņāüļÉ£ Ļ░üļ¦ēņŗĀĻ▓ĮņØä ĒÜīļ│Ąņŗ£ņ╝░ļŗżĻ│Ā ĒĢ£ John et al [32]ņØś ņŚ░ĻĄ¼ņÖĆļŖö ņ░©ņØ┤ļź╝ ļ│┤ņśĆļŗż. John et al [32]ņØś ņŚ░ĻĄ¼ļŖö ņĢłĻĄ¼Ļ▒┤ņĪ░ņ”Ø ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņŗ£Ē¢ēĒĢ£ ņŚ░ĻĄ¼ļĪ£ ļ│Ė ņŚ░ĻĄ¼ņÖĆ ļīĆņāüņØ┤ ļŗ¼ļØ╝ ņØ┤Ļ▓āņ£╝ļĪ£ ņØĖĒĢ£ ņ░©ņØ┤ļØ╝ ņāØĻ░üļÉ£ļŗż. ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ņ¦äļŗ© Ēøä ĒÅēĻĘĀ 120.2ņØ╝ ļÅÖņĢł ņ╣śļŻīņŚÉļÅä ņ╣śļŻī ĒÜ©Ļ│╝Ļ░Ć ņĀüņŚłļŹś ĒÖśņ×ÉļōżņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņ╣śļŻī Ēøä 2Ļ░£ņøö ņØ┤ļé┤ņŚÉ Ļ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØś ĒśĖņĀäņØä ļ│┤ņŚ¼ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņŚÉņä£ ĒÜ©Ļ│╝ņĀüņØ┤ņŚłļŗż.
ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ņ╣śļŻī ĒÜ©Ļ│╝ ņØ┤ņÖĖņŚÉļÅä ĻĖ░ņĪ┤ ņ╣śļŻī ļ░®ļ▓ĢĻ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ļŗżņ¢æĒĢ£ ņןņĀÉņØ┤ ņ׳ļŗż. ņ¢æļ¦ēņØ┤ņŗØņłĀņØĆ ņØ┤ņŗØļÉ£ ņ¢æļ¦ēņØ┤ ņĢłĻĄ¼Ēæ£ļ®┤ņŚÉ ļČĆņ░®ļÉśņ¢┤ ņ׳ļŖö ĻĖ░Ļ░ä ļÅÖņĢłļ¦ī ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ ņ╣śļŻī ĻĖ░Ļ░äņØ┤ ņĀ£ĒĢ£ņĀüņØ╝ ņłś ņ׳ņ¦Ćļ¦ī, ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ Ļ░üļ¦ēņåÉņāüņØ┤ ĒÜīļ│ĄļÉĀ ļĢīĻ╣īņ¦Ć ņé¼ņÜ®ĒĢĀ ņłś ņ׳ņ¢┤ ņśżļ×£ ĻĖ░Ļ░ä ļÅÖņĢł ļ¦ÄņØĆ ņä▒ņןņØĖņ×Éļź╝ ņåÉņāü ļ░øņØĆ Ļ░üļ¦ēņŚÉ ņĀ£Ļ│ĄĒĢĀ ņłś ņ׳ņ£╝ļ®░, ņ¢æļ¦ēņØ┤ņŗØņłĀĻ│╝ Ļ░ÖņØ┤ ņ╣©ņŖĄņĀüņØĖ ņŗ£ņłĀņØ┤ ĒĢäņÜöĒĢśņ¦Ć ņĢŖņĢä ĒåĄņ”Ø, ņłśņłĀ Ēøä ļČłĒÄĖĻ░É ļō▒ņØ┤ ņŚåļŗż. ņ×ÉĻ░ĆĒśłņ▓ŁņĢłņĢĮņØĆ ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖś ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ Ēśłņ▓ŁņŚÉ ņĪ┤ņ×¼ĒĢśļŖö pro-immune ĻĘĖļ”¼Ļ│Ā pro-inflammatory ņä▒ļČäņØ┤ ņ×ÉĻ░ĆĒśłņ▓ŁņĢłņĢĮņŚÉ ĒżĒĢ©ļÉśņ¢┤ ĒÜ©ļŖźņØä ņĀ£ĒĢ£ĒĢĀ ņłś ņ׳ņ¢┤ ĻĖ░ņĀĆņ¦łĒÖśņŚÉ ļö░ļØ╝ ņśüĒ¢źņØä ļ░øņØä ņłś ņ׳ņ¦Ćļ¦ī, ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ĒĢŁņŚ╝ņ”Ø ļ░Å ļ®┤ņŚŁņĪ░ņĀł ĒŖ╣ņä▒ņØ┤ ņ׳ņ¢┤ ļŹö ļŗżņ¢æĒĢ£ ĒÖśņ×ÉņŚÉņä£ ņĢłņĀĢņĀüņ£╝ļĪ£ ņé¼ņÜ® Ļ░ĆļŖźĒĢśĻ│Ā, ņ×ÉĻ░ĆĒśłņ▓ŁņĢłņĢĮņØĆ ņśżņŚ╝ļÉśĻĖ░ ņē¼ņ¢┤ ļ│┤Ļ┤ĆņØ┤ Ļ╣īļŗżļĪŁņ¦Ćļ¦ī ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ņāüņś©ņŚÉņä£ 2ņŻ╝ ļÅÖņĢł ļ│┤Ļ┤ĆņØ┤ Ļ░ĆļŖźĒĢśņŚ¼ Ļ┤Ćļ”¼Ļ░Ć ĒÄĖļ”¼ĒĢśļŗż[33,34]. ņĀ£ļīĆĒśłņ▓ŁņĢłņĢĮņØĆ ĒśłĒ¢ēņä▒ ņ¦łĒÖśņØś ņĀäĒīī, ņśżņŚ╝ņØś ņ£äĒŚśņØ┤ ņĪ┤ņ×¼ĒĢśļ®░, Ļ│ĄņŚ¼ņ×ÉņØś ļÅÖņØśĻ░Ć ļ░śļō£ņŗ£ ĒĢäņÜöĒĢśļŗżļŖö ņĀÉņØ┤ ņ׳ņ¦Ćļ¦ī, ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØĆ ņāüņÜ®ĒÖöļÉ£ ņĀ£ĒÆłņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņĀ£ņĪ░ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņ£äņÖĆ Ļ░ÖņØĆ ļ¼ĖņĀ£Ļ░Ć ņĀüļŗż[5]. ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØś ļŗ©ņĀÉņ£╝ļĪ£ļŖö ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØś ņĀ£ņĪ░ Ļ│╝ņĀĢņØ┤ Ēæ£ņżĆĒÖöļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖĻ│Ā, ņāüņÜ®ĒÖöļÉ£ ņĀ£ĒÆłņØ┤ ņ׳ņ¦Ćļ¦ī Ļ│ĄņŚ¼ņ×ÉņŚÉ ļö░ļØ╝ ņä▒ņןņØĖņ×É ļåŹļÅä ļō▒ņØ┤ ļŗżļź╝ ņłś ņ׳ņ¢┤ ņĀĢļ¤ēĒÖöĻ░Ć ļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖņ£╝ļ®░, ļÅÖĻ▓░Ļ▒┤ņĪ░ ļō▒ņØś ņĀ£ņĪ░ Ļ│╝ņĀĢņØä Ļ▒░ņ╣£ ĒøäņŚÉ ņä▒ņןņØĖņ×ÉņØś ļåŹļÅä ļō▒ņØś ļ│ĆĒÖöĻ░Ć ņ׳ņØä ņłś ņ׳ļŗżļŖö ņĀÉņØ┤ ņ׳ļŗż.
ļ│Ė ņŚ░ĻĄ¼ņØś ņĀ£ĒĢ£ņĀÉņ£╝ļĪ£ ņ▓½ņ¦Ė, ļīĆņĪ░ĻĄ░ņØ┤ ņŚåļŖö ņ×äņāü ņ”ØļĪĆ ņŚ░ĻĄ¼ņØĖ ņĀÉ, ļæśņ¦Ė, ļīĆņāüņ×É ņłśĻ░Ć ņĀüņ¢┤ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņØä ņ£Āļ░£ĒĢśļŖö ļ¦ÄņØĆ ņ¦łĒÖśņØä ļīĆĒæ£ĒĢĀ ņłś ņŚåĻ│Ā, ņ╣śļŻī Ļ▓░Ļ│╝ņŚÉ ļö░ļźĖ ņ×äņāüņĀü ņ░©ņØ┤ļź╝ ļ╣äĻĄÉĒĢĀ ņłś ņŚåņŚłļŹś ņĀÉĻ│╝ ņģŗņ¦Ė, ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņÖĖ ļŗżļźĖ ņĢłņĢĮņØś ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļ░░ņĀ£ĒĢĀ ņłś ņŚåļŖö ņĀÉņØ┤ ņ׳Ļ▓Āļŗż. ĒĢśņ¦Ćļ¦ī ļ│Ė ņŚ░ĻĄ¼ļŖö ņØ┤ņĀä ņŚ░ĻĄ¼ļ│┤ļŗż ļ¦ÄņØĆ ņłśņØś ĒÖśņ×ÉņÖĆ ļŗżņ¢æĒĢ£ ņ¦łĒÖśņØä ĒżĒĢ©ĒĢśņśĆĻ│Ā, ļé£ņ╣śņä▒ Ļ░üļ¦ēņāüĒö╝ņäĖĒżĻ▓░ņåÉņŚÉņä£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪņØ┤ ĒÜ©Ļ│╝ņĀüņ×äņØä ĒåĄĻ│äņĀüņ£╝ļĪ£ ļ│┤ņśĆļŗżļŖö ņĀÉņŚÉņä£ ņØśņØśĻ░Ć ņ׳ļŗż. ņČöĒøä ļŗżĻĖ░Ļ┤Ć ņĀäĒ¢źņĀü ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢśņŚ¼ ļŗżņ¢æĒĢ£ ņ¦łĒÖśņØä ĒżĒĢ©ĒĢśĻ│Ā, ņ╣śļŻī ĒÜ©Ļ│╝ņŚÉ ļö░ļźĖ ņ×äņāüņĀü ĒŖ╣ņ¦ĢņØä ļČäņäØĒĢśĻ│Ā, ĻĖ░ņĪ┤ ņĢĮņĀ£ Ļ░äņØś ĒÜ©ļŖź ļ╣äĻĄÉņÖĆ ļ│æĒĢ®ņÜöļ▓ĢņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļź╝ ņŗ£Ē¢ēĒĢ£ļŗżļ®┤ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņŚÉņä£ ņ╣śļŻī ļ░®ļ▓ĢĻ│╝ ĒÜ©ļŖźņØä ĒÅēĻ░ĆĒĢśļŖö ļŹ░ņŚÉ ļÅäņøĆņØ┤ ļÉĀ Ļ▓āņØ┤ļØ╝ ņāØĻ░üĒĢ£ļŗż. Ļ▓░ļĪĀņĀüņ£╝ļĪ£ ņ¢æļ¦ēņČöņČ£ļ¼╝ ņĀÉņĢłņĢĪ ņ╣śļŻīļŖö ĻĖ░ņĪ┤ ņ╣śļŻī ļ░®ļ▓ĢņŚÉ ĒśĖņĀäļÉśņ¦Ć ņĢŖņØĆ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉ ĒÖśņ×ÉņŚÉņä£ ņĢłĻĄ¼ ņ”ØņāüņØś ņÖäĒÖöņÖĆ Ļ░üļ¦ēņāüĒö╝ņåÉņāüņØś ĒÜīļ│ĄņŚÉ ļÅäņøĆņØä ņŻ╝ņŚłĻ│Ā, ļö░ļØ╝ņä£ ļé£ņ╣śņä▒ ņ¦ĆņåŹĻ░üļ¦ēņāüĒö╝Ļ▓░ņåÉņŚÉņä£ ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ Ļ│ĀļĀżĒĢĀ ņłś ņ׳Ļ▓Āļŗż.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






