

ņŗ£ņŗĀĻ▓ĮņŚ╝ņØĆ ņŗ£ņŗĀĻ▓ĮņØś ņŚ╝ņ”Ø ļ░Å Ēāłņłśņ┤łĒÖöļĪ£ ļ░£ņāØĒĢśļŖö ņ¦łĒÖśņ£╝ļĪ£, ņŻ╝ļĪ£ ļŗ©ņĢłņØś ĒåĄņ”ØņØä ļÅÖļ░śĒĢ£ ņŗ£ļĀźņĀĆĒĢś, ņŗ£ņĢ╝Ļ░Éņåī ļ░Å ņāēĻ░üņØ┤ņāüņ£╝ļĪ£ ļéśĒāĆļé£ļŗż. ņĀäĒśĢņĀüņØĖ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØĆ 20-40ļīĆ ņŚ¼ņ×ÉņŚÉņä£, ņĢłĻĄ¼ņÜ┤ļÅÖ ņŗ£ ņŗ¼ĒĢ┤ņ¦ĆļŖö ĒåĄņ”ØĻ│╝ ĒĢ©Ļ╗ś ļŗ©ņĢłņØś ņŗ£ļĀźņĀĆĒĢśĻ░Ć ņłśņØ╝ņŚÉ Ļ▒Ėņ│É ļ░£ņāØĒĢśļ®░ ņØ┤Ēøä ņä£ņä£Ē׳ ĒśĖņĀäļÉśļŖö ĒŖ╣ņ¦ĢņØä ļ│┤ņØĖļŗż. ĻĘĖ ņøÉņØĖņØĆ ļīĆļČĆļČä ņŚ╝ņ”Øņä▒ Ēāłņłśņ┤łĒÖöĻ░Ć ņ░©ņ¦ĆĒĢśĻ│Ā, ĻĘĖņÖĖ ļ░öņØ┤ļ¤¼ņŖż Ļ░ÉņŚ╝ņä▒ ņ¦łĒÖś, ļćīļ¦ēņØ┤ļéś ļłł ņŻ╝ņ£ä ņĪ░ņ¦ü ļ░Å ļČĆļ╣äļÅÖ ņŻ╝ņ£äņØś ņŚ╝ņ”ØņØś ĒīīĻĖē, ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖś ļō▒ņØ┤ ņ׳ļŗż[1].
Ļ▓░ĒĢĄņĢĮņĀ£ ņżæņŚÉņä£ EthambutolņŚÉ ņØśĒĢ£ ļÅģņä▒ņŗ£ņŗĀĻ▓Įļ│æņ”ØņØĆ ļäÉļ”¼ ņĢīļĀżņĀĖ ņ׳ņ¢┤ Ļ▓░ĒĢĄņ╣śļŻī ņżæ ņŗ£ļĀźņĀĆĒĢśĻ░Ć ļ░£ņāØĒĢĀ Ļ▓ĮņÜ░ ņĢĮņĀ£ļź╝ ņżæļŗ©ĒĢśĻ│Ā ļé┤ņøÉĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ĒØöĒ׳ ņ׳ļŗż[2]. ĻĘĖļ¤¼ļéś ĻĘĖ ņÖĖņØś ņĢĮņĀ£ļōżņØ┤ ņŗ£ņŗĀĻ▓ĮņŚÉ ļ»Ėņ╣Ā ņłś ņ׳ļŖö ņśüĒ¢źņŚÉ ļīĆĒĢ┤ņä£ļŖö ļ│┤Ļ│ĀĻ░Ć ļ¦Äņ¦Ć ņĢŖĻ│Ā, ņØ┤ņŚÉ ļīĆĒĢ£ ĻĄÉņ£ĪņØ┤ ļČĆņĪ▒ĒĢ£ ņŗżņĀĢņØ┤ļŗż.
ņóģņ¢æĻ┤┤ņé¼ņØĖņ×É(tumor necrosis factor, TNF)-╬▒ņŚÉ ļīĆĒĢ£ ļŗ©ņØ╝ Ēü┤ļĪĀņä▒ ĒĢŁņ▓┤ņØĖ infliximab (Remicade┬«, Schering-Plough, Welwyn Garden City, UK)ņØĆ TNF-╬▒ņŚÉ Ļ▓░ĒĢ®ĒĢśņŚ¼ ņŚ╝ņ”Øļ░śņØæņØä ņ¢ĄņĀ£ĒĢśņŚ¼ Ēü¼ļĪĀļ│æ, ņŚ╝ņ”Øņä▒ ņןņ¦łĒÖś, ļźśļ¦łĒŗ░ņŖżņä▒ Ļ┤ĆņĀłņŚ╝ ļō▒ņØś ņĀäņŗĀ ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖśņØś ņ╣śļŻīņĀ£ļĪ£ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ņ£╝ļ®░[3,4], ņĢłĻ│╝ņĀüņ£╝ļĪ£ļŖö ĒżļÅäļ¦ēņŚ╝, Ļ│Ąļ¦ēņŚ╝ ļō▒ ļ¦īņä▒ ņ×¼ļ░£ņä▒ ņŚ╝ņ”Øņ¦łĒÖśņŚÉņä£ ņ╣śļŻī ĒÜ©Ļ│╝Ļ░Ć ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż[4].
ļ░śļ®┤ TNF-╬▒ ņ¢ĄņĀ£ņĀ£ļŖö ņŗĀĻ▓ĮĻ│äĒåĄņØś Ēāłņłśņ┤łĒÖöļź╝ ņ£Āļ░£ĒĢśņŚ¼, ņŗ£ņŗĀĻ▓ĮņŚ╝, ļŗżļ░£Ļ▓ĮĒÖöņ”Ø ļō▒ņØś ļČĆņ×æņÜ®ņØä ļ░£ņāØņŗ£Ēé¼ ņłś ņ׳ļŗż[5]. ĻĘĖļ¤¼ļéś, ĻĄŁļé┤ņŚÉņä£ļŖö ņĢäņ¦üĻ╣īņ¦Ć infliximabĻ│╝ Ļ┤ĆļĀ©ĒĢ£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņŚÉ ļīĆĒĢ£ ļ│┤Ļ│ĀĻ░Ć ņŚåņ¢┤, ņĀĆņ×ÉļōżņØĆ Ēü¼ļĪĀļ│æņŚÉņä£ ņŻ╝ĻĖ░ņĀüņ£╝ļĪ£ TNF-╬▒ ņ╣śļŻīļź╝ ļ░øņĢäņś© ņĀŖņØĆ ļé©ņ×ÉņŚÉņä£ ņĢĮņĀ£ņÖĆ Ļ┤ĆļĀ©ļÉ£ Ļ▓āņ£╝ļĪ£ ņØśņŗ¼ņØ┤ ļÉśļŖö ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢśņŚ¼ ņ╣śļŻīĒĢ£ Ļ▓ĮņÜ░ļź╝ Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ņØ┤ļź╝ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”ØļĪĆļ│┤Ļ│Ā
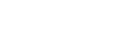
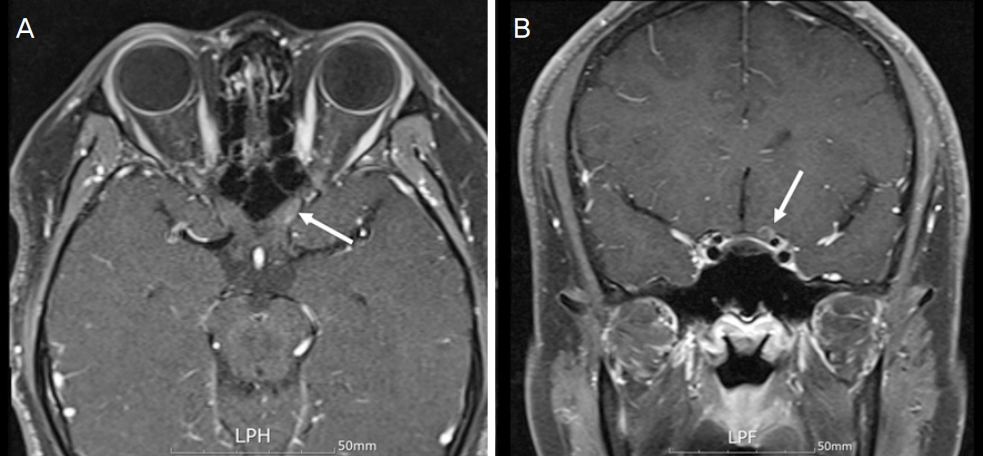
22ņäĖ ļé©ņ×É ĒÖśņ×ÉĻ░Ć 2-3ņŻ╝ ņĀäļČĆĒä░ ņóīņĢłņØś ņŗ£ņĢ╝Ļ░Ć ĒØÉļĀżņ¦ĆļŖö ņ”Øņāüņ£╝ļĪ£ ļ│ĖņøÉ ņØæĻĖēņŗżļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀźņØĆ ņÜ░ņĢł 1.0, ņóīņĢł 0.4ļĪ£ ņĖĪņĀĢļÉśņŚłĻ│Ā, ļÅÖĻ│ĄļČĆļō▒ņØĆ ņŚåņŚłņ£╝ļ®░, ņóīņĢłņØś ņāüļīĆĻĄ¼ņŗ¼ļÅÖĻ│ĄņÜ┤ļÅÖņןņĢĀĻ░Ć Ļ▓Įļ»ĖĒĢśĻ▓ī Ļ┤Ćņ░░ļÉśņŚłļŗż. ņĢłĻĄ¼ņÜ┤ļÅÖņŗ£ņØś ņ£Āļ░£ļÉśļŖö ĒåĄņ”ØņØĆ ņŚåņŚłĻ│Ā, ņāēĻ░üĻ▓Ćņé¼ņŚÉņä£ ņÜ░ņĢłņØĆ 21Ļ░£ ļ¬©ļæÉ, ņóīņĢłņØĆ 21Ļ░£ ņżæ 12Ļ░£ļź╝ ļ¦×ņČöņ¢┤ ņāēĻ░üņØ┤ ņĀĆĒĢśļÉśņ¢┤ ņ׳ņŚłņ£╝ļ®░, ņŗ£ņĢ╝Ļ▓Ćņé¼ņāüņŚÉņä£ ņóīņĢłņØś ņżæņŗ¼ĒĢśņĖĪņØś ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ļ│┤ņśĆļŗż(Fig. 1A). ņĢłņĀĆĻ▓Ćņé¼ņāü ņŗ£ņŗĀĻ▓Įņ£ĀļæÉ ļ░Å ļ¦Øļ¦ēņŚÉļŖö ĒŖ╣ņØ┤ ņåīĻ▓¼ņØ┤ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśņ£╝ļ®░, ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśüņŚÉņä£ ĒÖ®ļ░śļČĆ ņŗĀĻ▓ĮņĀłņäĖĒż-ļé┤ļ¦ØņāüņĖĄ(ganglion cell-inner plexiform layer)ņØś ļæÉĻ╗śĻ░Ć Ļ░ÉņåīļÉśņ¢┤ ņ׳ņŚłļŗż(Fig. 1B). ņŗ£ņŗĀĻ▓Įļ│æņ”ØņØś ņøÉņØĖ Ļ░Éļ│äņØä ņ£äĒĢ┤ ņŗ£Ē¢ēĒĢ£ ņĢłņÖĆ ņ×ÉĻĖ░Ļ│Ąļ¬ģņśüņāü(magnetic resonance imaging, MRI)ņŚÉņä£ ņóīņĖĪ ņŗ£ņŗĀĻ▓ĮņØś ņĢłņÖĆļé┤, Chiasm ņĢ×ņ¬Į ņĪ░ņśüņ”ØĻ░ĢņØ┤ ļ│┤ņśĆĻ│Ā, ļćīņŗżņ¦łņØś ļŗżļźĖ ļ¼ĖņĀ£ļŖö Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 2). ņ£ĀņĀäņä▒ ņŗ£ņŗĀĻ▓Įļ│æņ”Ø ĒÖĢņØĖņØä ņ£äĒĢ┤ ņŗ£Ē¢ēĒĢ£ leber hereditary optic neuropathy ņ£ĀņĀäņ×É(LHON gene)ļŖö Ļ▓ĆņČ£ļÉśņ¦Ć ņĢŖņĢśļŗż. ĒÖśņ×ÉļŖö Ēü¼ļĪĀļ│æņ£╝ļĪ£ ĒāĆļ│æņøÉņŚÉņä£ 2016ļģäļČĆĒä░ infliximab (Remicade┬«, Schering-Plough) ņ╣śļŻīļź╝ ļ░øļŹś ļČäņ£╝ļĪ£, 2019ļģäļČĆĒä░ļŖö ņÜ®ļ¤ēņØä ļæÉ ļ░░ļĪ£ ņ”Øļ¤ēĒĢśņŚ¼ 2Ļ░£ņøöļ¦łļŗż 600 mg (10 mg/kg)ņ£╝ļĪ£ ņĀĢļ¦źņŻ╝ņé¼ ņ╣śļŻīļź╝ ļ░øņĢśņ£╝ļ®░, ņÜ®ļ¤ē ņ”ØĻ░ĆĒĢ£ Ēøä 8ļ▓łņ¦Ė ņŻ╝ņé¼ļź╝ ļ¦×Ļ│Ā ļé£ Ēøä 2ņØ╝ņ¦Ė ņŗ£ļĀźņĀĆĒĢś ņ”ØņāüņØ┤ ņŗ¼ĒĢ┤ņĀĖ ļ│ĖņøÉ ņØæĻĖēņŗżļĪ£ ļé┤ņøÉĒĢśņśĆļŗż. ņØ┤ņŚÉ, infliximabĻ│╝ ņŚ░Ļ┤ĆļÉ£ ĻĄ¼Ēøäņŗ£ņŗĀĻ▓ĮņŚ╝ņØä ņØśņŗ¼ĒĢśĻ│Ā, Ļ│ĀņÜ®ļ¤ēņŖżĒģīļĪ£ņØ┤ļō£ 1 g ņĀĢļ¦źņŻ╝ņé¼ļź╝ 3ņØ╝ ļÅÖņĢł ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, 3ņØ╝ņ¦Ė ņĄ£ļīĆĻĄÉņĀĢņŗ£ļĀźņØĆ 0.8ļĪ£ ĒśĖņĀäļÉśņŚłĻ│Ā, Ļ▓ĮĻĄ¼ņĢĮņ£╝ļĪ£ Ļ░Éļ¤ēĒĢśļ®┤ņä£ ņ╣śļŻī 1Ļ░£ņøöņ¦Ė ņŗ£ļĀźņØĆ 1.0ņ£╝ļĪ£, ņāēĻ░ü ļ░Å ņŗ£ņĢ╝ļŖö ļČĆļČäņĀüņ£╝ļĪ£ ĒśĖņĀäņØ┤ ļÉśņŚłņ£╝ļ®░, ņ╣śļŻī 3Ļ░£ņøöņ¦ĖņŚÉļŖö ļ¬©ļæÉ ĒśĖņĀäļÉśņŚłļŗż(Fig. 3). ņ╣śļŻī 2Ļ░£ņøöņ¦ĖņŚÉļŖö infliximab ņŻ╝ņé¼ ņ╣śļŻīļź╝ ņ×¼ņŗ£ņ×æĒĢśņśĆņ£╝ļéś, Ēśäņ×¼Ļ╣īņ¦Ć ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ņ×¼ļ░£ ņ¢æņāüņØĆ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗż.
Ļ│Ā ņ░░
ņóģņ¢æĻ┤┤ņé¼ņØĖņ×ÉļŖö 1975ļģä ņĢöņäĖĒżļź╝ ņäĀĒāØņĀüņ£╝ļĪ£ Ļ┤┤ņé¼ņŗ£ĒéżļŖö ņé¼ņØ┤ĒåĀņ╣┤ņØĖņ£╝ļĪ£ ņ▓śņØī ņåīĻ░£ļÉ£ ņØ┤Ēøä, ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć Ļ░ÉņŚ╝ņØ┤ļéś ņóģņ¢æņŚÉ ļīĆĒĢ£ ņĀĢņāüņĀüņØĖ ņŚ╝ņ”Øļ░śņØæ ļ░Å ļ®┤ņŚŁņ▓┤Ļ│äņŚÉņä£ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ļŗ┤ļŗ╣ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ĻĘĖļ¤¼ļéś ņŚ╝ņ”Øņä▒ ņ¦łĒÖśņŚÉņä£ļŖö ņØ┤ļ¤¼ĒĢ£ TNFĻ░Ć ļČĆņĀüņĀłĒĢśĻ▓ī Ļ│╝ļÅä ņāØņé░ļÉĀ Ļ▓ĮņÜ░ ļ®┤ņŚŁņ▓┤Ļ│äņØś ļŗżņ¢æĒĢ£ ņäĖĒżļź╝ ĒÖ£ņä▒ĒÖöņŗ£ņ╝£ ņäĖĒż ļÅģņä▒ ĒÜ©Ļ│╝ļź╝ ņ£Āļ░£ĒĢśĻ│Ā, ņĪ░ņ¦üņØś ņåÉņāüņØä ņĢ╝ĻĖ░ĒĢĀ ņłś ņ׳ļŗż[3].
ņóģņ¢æĻ┤┤ņé¼ņØĖņ×É ņ¢ĄņĀ£ņĀ£(TNF-╬▒ inhibitor)Ļ░Ć ņŚ╝ņ”Øļ░śņØæņØś Ļ░ĢļĀźĒĢ£ ļ¦żĻ░£ņ▓┤ņØĖ TNF-╬▒ņØś ņ×æņÜ®ņØä ņ¢ĄņĀ£ņŗ£Ēé┤ņ£╝ļĪ£ņŹ©, ļ¦īņä▒ ņŚ╝ņ”Øļ░śņØæņØä Ļ░Éņåīņŗ£ĒéżĻ│Ā, ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖśņØä ĒśĖņĀäņŗ£Ēé¼ ņłś ņ׳ļŗżļŖö Ļ▓āņØ┤ ļ░ØĒśĆņ¦Ćļ®┤ņä£, ļźśļ¦łĒŗ░ņŖżņä▒ Ļ┤ĆņĀłņŚ╝, Ļ░Ģņ¦üņä▒ ņ▓ÖņČöņŚ╝, Ļ▒┤ņäĀ Ļ┤ĆņĀłņŚ╝, ņŚ╝ņ”Øņä▒ ņןņ¦łĒÖś, ĒżļÅäļ¦ēņŚ╝ ļō▒ņŚÉņä£ ĒÜ©Ļ│╝ņĀüņ£╝ļĪ£ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ļŗż[4]. Ēśäņ×¼Ļ╣īņ¦Ć ņāüņÜ®ĒÖöļÉśĻ│Ā ņ׳ļŖö TNF-╬▒ ņ¢ĄņĀ£ņĀ£ļŖö infliximab (Remicade┬«, Schering-Plough), etanercept (Enbrel┬«), adalimumab (Humira┬«), golimumab (Simponi┬«), certolizumab (Cimzia┬«) 5Ļ░Ćņ¦Ć ņóģļźśĻ░Ć ņ׳ņ£╝ļ®░[6], ņØ┤ļōżņØĆ ņĀäĒåĄņĀüņØĖ ĒĢŁļźśļ¦łĒŗ░ņŖż ņĢĮņĀ£ņØĖ methotrexate, hydroxychloroquine, sulfasalazine ļō▒ disease modifying antirheumatic drugs (DMARDs)ņØś ņ╣śļŻīņŚÉļÅä ĒÜ©Ļ│╝Ļ░Ć ļ»ĖĒØĪĒĢĀ Ļ▓ĮņÜ░ ņé¼ņÜ®ļÉśļ®░, Ļ░Ćņן ĒÜ©Ļ│╝Ļ░Ć ņóŗņØĆ ĒĢŁļźśļ¦łĒŗ░ņŖż ņ╣śļŻīņĀ£ļĪ£ņä£ ĻĄ¼ņĪ░ņĀüņØĖ ņåÉņāüņØś ļ░£ņāØņØä ņśłļ░®ĒĢ┤ņŻ╝ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĪīļŗż[7]. ĻĘĖļ¤¼ļéś, ņØ┤ļ¤¼ĒĢ£ ņ£ĀņÜ®ņä▒ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņĀäņŗĀņä▒ ļŻ©ĒæĖņŖż, ĒśłĻ┤ĆņŚ╝ ļō▒ņØś ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖśņØś ļ░£ņāØ, Ļ▓░ĒĢĄņØś ņ£äĒŚśļÅä ņ”ØĻ░Ć, ņ╣©ņ£żņä▒ ņ¦äĻĘĀ Ļ░ÉņŚ╝ņØś ļ░£ņāØ, ņÜĖĒśłņä▒ ņŗ¼ļČĆņĀäņØś ņĢģĒÖö, Ļ░äļÅģņä▒, ļ”╝Ēöäņóģ ļō▒ ņóģņ¢æ ļ░£ņāØ ņ£äĒŚśļÅä ņ”ØĻ░ĆņÖĆ ĒĢ©Ļ╗ś ņżæņČöņŗĀĻ▓ĮĻ│äņØś Ēāłņłśņ┤łĒÖöņÖĆ Ļ┤ĆļĀ©ļÉ£ ļČĆņ×æņÜ®ņØĖ ņŗ£ņŗĀĻ▓ĮņŚ╝, ļ¦īņä▒ ņŚ╝ņ”Øņä▒ Ēāłņłśņ┤łņä▒ ļŗżļ░£ņä▒ ņŗĀĻ▓Įļ│æņ”Ø, ĻĖĖļ”¼ņĢł ļ░öļĀł ņ”ØĒøäĻĄ░ ļō▒ņØś ļČĆņ×æņÜ®ņØ┤ ļ│┤Ļ│ĀļÉśņŚłļŗż[5,8,9]. ĻĘĖ ņÖĖņŚÉ ņĢłĻ│╝ņĀüņ£╝ļĪ£ļŖö ņŚ╝ņ”Øņä▒ ļłł ņ¦łĒÖś, ĒżļÅäļ¦ēņŚ╝, Ļ│Ąļ¦ēņŚ╝, ņÖĖņĢłĻĘ╝ņŚ╝, ņĢłļé┤ņŚ╝, ļ¦Øļ¦ēĒśłĻ┤ĆņŚ╝, ņé¼ļź┤ņĮöņØ┤ļō£ ļō▒ņØś ļČĆņ×æņÜ®ņØ┤ ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ļŗż[6].
TNF ņ¢ĄņĀ£ņĀ£ ņé¼ņÜ®Ļ│╝ Ļ┤ĆļĀ©ļÉ£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņŚÉ ļīĆĒĢ£ ļ│┤Ļ│ĀļŖö 2002ļģä ņØ┤Ēøä Ēśäņ×¼Ļ╣īņ¦Ć Pubmed Ļ▓ĆņāēņØä ĒĢ£ Ļ▓░Ļ│╝ 43ņśłĻ░Ć ļ│┤Ļ│ĀļÉśņŚłĻ│Ā[10-37], ņØ┤ ņżæ infliximab Ļ┤ĆļĀ©ļÉ£ ļ│┤Ļ│ĀĻ░Ć 21ņśł, etanercept Ļ┤ĆļĀ©ĒĢśņŚ¼ 6ņśł, adalimumab Ļ┤ĆļĀ© 5ņśł, golimumab Ļ┤ĆļĀ© 1ņśłĻ░Ć ĒżĒĢ©ļÉśņŚłļŗż. ņŗ£ņŗĀĻ▓ĮļČĆņóģņØä ļÅÖļ░śĒĢ£ Ēāłņłśņ┤łņä▒ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ 17ņśł, ņŗ£ņŗĀĻ▓Įņ£ĀļæÉņØś ļ│ĆĒÖöļź╝ ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŹś ĻĄ¼Ēøäņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ĒśĢĒā£Ļ░Ć 18ņśł, ĻĘĖ ņÖĖ ļÅģņä▒ņŗ£ņŗĀĻ▓Įļ│æņ”ØņØ┤ 4ņśł ĒżĒĢ©ļÉśņŚłĻ│Ā, ņŗ£ņŗĀĻ▓ĮņŚ╝ ĒśĢĒā£ņŚÉ ļīĆĒĢ£ ņ¢ĖĻĖēņØ┤ ņŚåļŖö ļ│┤Ļ│ĀļÅä ĒżĒĢ©ļÉśņŚłļŗż. Ļ│ĀņÜ®ļ¤ē ņŖżĒģīļĪ£ņØ┤ļō£ ņĀĢļ¦źņŻ╝ņé¼ļź╝ ņŗ£Ē¢ēĒĢ£ Ļ▓ĮņÜ░Ļ░Ć 31ņśł, Ļ▓ĮĻĄ¼ņŖżĒģīļĪ£ņØ┤ļō£ ļ│ĄņÜ®ĒĢ£ Ļ▓ĮņÜ░Ļ░Ć 5ņśł, ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņØĆ Ļ▓ĮņÜ░Ļ░Ć 3ņśł ņ׳ņŚłĻ│Ā, ņŗ£ļĀźņØ┤ ļ¬©ļæÉ ĒśĖņĀäļÉ£ Ļ▓ĮņÜ░Ļ░Ć 20ņśł, ļČĆļČäņĀüņ£╝ļĪ£ ĒśĖņĀäļÉ£ Ļ▓ĮņÜ░Ļ░Ć 13ņśł, ĒśĖņĀäņØ┤ ņŚåņŚłļŹś Ļ▓ĮņÜ░Ļ░Ć 10ņśłĻ░Ć ņ׳ņŚłļŗż. ņØ┤ ņżæ ņ╣śļŻī ņŚåņØ┤ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ņØä ņŗ£Ē¢ēĒĢ£ 3ņśł ļ¬©ļæÉ 3Ļ░£ņøö ņØ┤ļé┤ ņÖäņĀä ĒÜīļ│ĄļÉśņŚłļŗż(Table 1).
Safety assessment of biologic ThERapy studyņŚÉ ļö░ļź┤ļ®┤, DMARDļź╝ ņé¼ņÜ®ĒĢśļŖö ĻĄ░Ļ│╝ TNF-╬▒ ņ¢ĄņĀ£ņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö ĻĄ░ņŚÉņä£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ļ░£ņāØ ļ╣łļÅäĻ░Ć ļ╣äņŖĘĒĢśļ»ĆļĪ£, TNF-╬▒ ņ¢ĄņĀ£ņĀ£ņØś ņé¼ņÜ®ņØ┤ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ļ░£ļ│æņØä ņ┤ēņ¦äņŗ£Ēé©ļŗżļŖö ĻĘ╝Ļ▒░Ļ░Ć ņŚåļŗżĻ│Ā ĒĢśņśĆļŗż[38]. ņØ┤ņÖĆ ļ░śļīĆļĪ£, 2014ļģä ņĀäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ 77ļ¬ģņØś ĒÖśņ×ÉņŚÉņä£ TNF-╬▒ ņ¢ĄņĀ£ņĀ£ ņ╣śļŻī ņĀäĒøä ņŗĀĻ▓ĮĒĢÖņĀü ņØ┤ņāü ņŚ¼ļČĆļź╝ ĒÖĢņØĖĒĢ£ Ļ▓░Ļ│╝, ņ╣śļŻī Ēøä ņŗĀĻ▓ĮĒĢÖņĀü ļČĆņ×æņÜ®ņØ┤ 3ļ¬ģņŚÉņä£ ļéśĒāĆļé¼ņ£╝ļ®░, ņØ┤ ņżæ 2ļ¬ģņŚÉņä£ ņ╣śļŻī ņżæļŗ©Ļ│╝ ĒĢ©Ļ╗ś ĒśĖņĀäļÉśņŚłļŗżĻ░Ć, ņ╣śļŻī ņ×¼ņŗ£ņ×æĻ│╝ ĒĢ©Ļ╗ś ļČĆņ×æņÜ®ņØ┤ ņ×¼ļ░£ĒĢśņŚ¼, TNF-╬▒ ņ¢ĄņĀ£ņĀ£ņØś ņ╣śļŻīĻ░Ć Ēāłņłśņ┤łĒÖöļź╝ ņ£Āļ░£ĒĢśņŚ¼, ņŗĀĻ▓ĮĻ│äĒåĄ ļČĆņ×æņÜ®ņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗżĻ│Ā ĒĢśņśĆļŗż[39].
ļ│Ė ņ”ØļĪĆ ĒÖśņ×ÉņŚÉņä£ ņŗ£Ļ░äņāü ņÜ░ņŚ░ņØś ņØ╝ņ╣śļĪ£ ņĢĮņĀ£ļź╝ ņé¼ņÜ®ĒĢśļŖö ĒÖśņ×ÉņŚÉņä£ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØ┤ ļ░£ņāØĒĢśņśĆņØä Ļ░ĆļŖźņä▒ņØä ņÖäņĀäĒ׳ ļ░░ņĀ£ĒĢśĻĖ░ļŖö ņ¢┤ļĀżņÜ░ļéś, ņĢłĻĄ¼ņÜ┤ļÅÖ ņŗ£ ĒåĄņ”ØņØ┤ ņŚåļŗżļŖö ņĀÉņŚÉņä£ ņĀäĒśĢņĀüņØĖ ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ņ”ØņāüņØä ļö░ļź┤ņ¦Ć ņĢŖņĢśĻ│Ā, ņŗ£ļĀźņĀĆĒĢśĻ░Ć ņŗ¼ĒĢ┤ņ¦ä ņŗ£ņĀÉņØ┤ infliximab ņŻ╝ņé¼ņ╣śļŻī 2ņØ╝ ļÆżņśĆļŗżļŖö ņĀÉņŚÉņä£, ņĢĮņĀ£ Ļ┤ĆļĀ© Ļ░ĆļŖźņä▒ņØä ņŚ╝ļæÉņŚÉ ļæś ņłś ņ׳ņŚłļŗż.
ļŗ©ņĢłņØś ņŗ£ļĀź ļ░Å ņāēĻ░üņĀĆĒĢśņÖĆ ņŗ£ņĢ╝Ļ▓░ņåÉņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉņä£ ņĢłņĀĆĻ▓Ćņé¼ņāü ņØ┤ņāüņØ┤ ņŚåņ£╝ļ®┤ņä£ ņāüļīĆĻĄ¼ņŗ¼ļÅÖĻ│ĄņÜ┤ļÅÖņןņĢĀĻ░Ć ņ׳ļŖö Ļ▓ĮņÜ░ ĻĄ¼Ēøäņŗ£ņŗĀĻ▓ĮņŚ╝, ļÆżĒŚłĒśłņŗ£ņŗĀĻ▓Įļ│æņ”Ø, ņĢĢļ░Ģņŗ£ņŗĀĻ▓Įļ│æņ”Ø ļō▒ņØä Ļ░Éļ│äĒĢ┤ņĢ╝ ĒĢ£ļŗż. ļ│Ė ņ”ØļĪĆņØś Ļ▓ĮņÜ░ ņŗ£ļĀźņĀĆĒĢśĻ░Ć ĻĖēņä▒ņ£╝ļĪ£ ļ░£ņāØĒĢśņ¦Ć ņĢŖņĢśĻ│Ā, Ļ│ĀĒśłņĢĢ, ļŗ╣ļć©, Ļ│ĀļĀ╣ ļō▒ ņ£äĒŚśņØĖņ×ÉņÖĆ ļ¦×ņ¦Ć ņĢŖņĢä ļÆżĒŚłĒśłņŗ£ņŗĀĻ▓Įļ│æņ”ØņØä ļ░░ņĀ£ĒĢśņśĆļŗż. ņĢłĻĄ¼ņÜ┤ļÅÖ ņŗ£ ĒåĄņ”ØņØ┤ ņŚåņŚłĻ│Ā, ĒśłņĢĪ Ļ▓Ćņé¼ņāü ņĀüĒśłĻĄ¼ ņ╣©Ļ░Ģ ņåŹļÅä(erythrocyte sedimentation rate), C-ļ░śņØæņä▒ ļŗ©ļ░▒ ņŗ£ĒŚś(C-reactive protein) ņāüņŖ╣ ļō▒ņØś ņŚ╝ņ”Ø ņāüĒā£ļź╝ ņŗ£ņé¼ĒĢśļŖö ņåīĻ▓¼ņØ┤ ņŚåņŚłņ£╝ļ®░, MRIņŚÉņä£ ņĢĢļ░Ģņä▒ ļ│æļ│Ć ņŚåņØ┤ ĻĄ¼Ēøäņŗ£ņŗĀĻ▓ĮņŚÉ ņĪ░ņśüņ”ØĻ░Ģ ņåīĻ▓¼ņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā, ņĢĮņĀ£ ņé¼ņÜ®ņØś ļ│æļĀźņ£╝ļĪ£ ļ»ĖļŻ©ņ¢┤ ļ│┤ņĢä, infliximab Ļ┤ĆļĀ© ņŗ£ņŗĀĻ▓ĮņŚ╝ņ£╝ļĪ£ ĒīÉļŗ©ĒĢśņśĆļŗż. ļÅģņä▒ ņŗ£ņŗĀĻ▓Įļ│æņ”ØņØ┤ļéś ņśüņ¢æ ņŗ£ņŗĀĻ▓Įļ│æņ”ØņØĆ ļ»ĖĒåĀņĮśļō£ļ”¼ņĢä ĻĖ░ļŖźņןņĢĀļź╝ ņ£Āļ░£ĒĢśņŚ¼ ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳Ļ│Ā, ņ¢æņĢłņä▒ņØĖ Ļ▓ĮņÜ░Ļ░Ć ļ¦ÄĻ│Ā, ļ¼┤ĒåĄņä▒ ņŗ£ļĀźņĀĆĒĢś ļ░Å ņāēĻ░üņĀĆĒĢśĻ░Ć ņ¦äĒ¢ēņä▒ņ£╝ļĪ£ ļ░£ņāØĒĢśļ®░, ņ£ĀļæÉĒÖ®ļ░śņŗĀĻ▓Įņä¼ņ£Āļŗżļ░£(papillomacular bundle)ņØś ņåÉņāüņ£╝ļĪ£ ņżæņŗ¼(central) ļśÉļŖö ļ¦╣ņĀÉņżæņŗ¼ņĢöņĀÉ(cecocentral scotoma)ņØä ņ£Āļ░£ĒĢśļŖö ĒŖ╣ņ¦ĢņØ┤ ņ׳ļŗż. ņŗ£ļĀźņØĆ ņłśņŻ╝ Ēś╣ņØĆ ņłśĻ░£ņøöņŚÉ Ļ▒Ėņ│É ņä£ņä£Ē׳ ĒÜīļ│ĄļÉśļ®░, ļÅģņä▒ņØä ņØ╝ņ£╝Ēé© ļ¼╝ņ¦łņØś ņóģļźśļéś ņ¢æ, ņåÉņāüņØś ņĀĢļÅäņŚÉ ļö░ļØ╝, ņśüĻĄ¼ņĀüņØĖ ņŗ£ļĀźņןņĢĀļź╝ ļé©ĻĖ░ĻĖ░ļÅä ĒĢ£ļŗż[39]. ļ│Ė ņ”ØļĪĆņØś Infliximab Ļ┤ĆļĀ© ņŗ£ņŗĀĻ▓ĮņŚ╝ņØĆ ļŗżļźĖ ņĢĮņĀ£ Ļ┤ĆļĀ© ļÅģņä▒ņŗ£ņŗĀĻ▓Įļ│æņ”ØĻ│╝ļŖö ļŗ©ņĢłņä▒ņØ┤ļØ╝ļŖö ņĀÉ, ņŗ£ļĀźĒÜīļ│ĄņØ┤ ļ╣Āļź┤ļŗżļŖö ņĀÉņŚÉņä£ ņ░©ņØ┤ņĀÉņØ┤ ņ׳ņŚłļŗż.
TNF ņ¢ĄņĀ£ņĀ£ Ļ┤ĆļĀ© ņŗ£ņŗĀĻ▓ĮņŚ╝ņ£╝ļĪ£ ņ¦äļŗ©ļÉ£ Ļ▓ĮņÜ░, ņØ┤ņĀä ļ│┤Ļ│ĀļōżņŚÉņä£ ņøÉņØĖņØ┤ ļÉśļŖö ņĢĮņĀ£ļź╝ ņżæļŗ©ĒĢśĻ│Ā ņŖżĒģīļĪ£ņØ┤ļō£ Ļ│ĀņÜ®ļ¤ē ņ╣śļŻīļź╝ ĒĢ£ Ēøä, ņøÉļלņØś ņ¦łĒÖś ņ╣śļŻīļź╝ ņ£äĒĢ┤ ļŗżļźĖ ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ļĪ£ ņĢĮņĀ£ļź╝ ļ│ĆĻ▓ĮĒĢśļŖö Ļ▓āņØä Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗżĻ│Ā ĒĢśņśĆņ£╝ļ®░, ļīĆĻ░£ ņ╣śļŻī Ēøä 1-3Ļ░£ņøöņ¦Ė ņŗ£ļĀź ļ░Å ņŗ£ĻĖ░ļŖźņØ┤ ĒÜīļ│ĄļÉ£ļŗżĻ│Ā ĒĢśņśĆļŗż[10-12,40]. ņŗ£ņŗĀĻ▓ĮņŚ╝ņØś ļ░£ņāØņØ┤ TNF-╬▒ ņ¢ĄņĀ£ņĀ£ ņ╣śļŻīņŚÉ ņØśĒĢ£ Ēāłņłśņ┤łĒÖöņŚÉņä£ ĻĖ░ņØĖĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£, ņŗ£ņŗĀĻ▓ĮņŚ╝ ĒÖśņ×É ļé┤ņøÉ ņŗ£ ņ×ÉņäĖĒĢ£ ļ│æļĀźņ▓ŁņĘ©ļź╝ ĒåĄĒĢśņŚ¼ ņĢĮņĀ£ Ļ┤ĆļĀ© ņ£Āļ¼┤ļź╝ ĒīÉļŗ©ĒĢśĻ│Ā, ņØ┤ņÖĆ Ļ┤ĆļĀ©ļÉ£ ņ¦łĒÖśņ£╝ļĪ£ ņØśņŗ¼ļÉśļŖö Ļ▓ĮņÜ░ ĒāĆĻ│╝ņÖĆņØś Ēśæņ¦äņØä ĒåĄĒĢ┤ TNF-╬▒ ņ¢ĄņĀ£ņĀ£ņØś ņé¼ņÜ® ņżæļŗ©ņØä Ļ│ĀļĀżĒĢśļ®┤ Ļ│ĀņÜ®ļ¤ē ņŖżĒģīļĪ£ņØ┤ļō£ ņ╣śļŻīļź╝ ĒĢ©ņ£╝ļĪ£ņŹ© ņ¢æĒśĖĒĢ£ ņŗ£ļĀźĒÜīļ│ĄņØä ĻĖ░ļīĆĒĢĀ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






