시신경주위염으로 발현된 사르코이드증
Optic Perineuritis as a Presenting Sign of Sarcoidosis
Article information
Abstract
목적
시신경주위염으로 발현된 사르코이드증을 보고하고자 한다.
증례요약
57세 남자가 2주 전 시작된 좌안 시력저하를 주소로 내원하였다. 환자는 1년 6개월 전 무증상 좌측 시신경주위염으로 한달간 경구 프레드니솔론을 복용한 후 호전된 병력이 있었다. 이번에는 눈운동 시 좌안 통증을 호소하였고, 좌안 교정시력은 20/50으로 저하되었으며 좌안에 색각이상과 상대구심동공운동장애가 관찰되었다. 전안부검사에서 특이 소견은 없었다. 안저검사에서 좌안시신경부종이 확인되었고, 안와자기공명영상에서 좌측 시신경주위의 조영증강 소견이 관찰되었다. 혈액검사에서 호산구양이온단백과 안지오텐신전환효소가 상승하였으며 흉부 방사선검사에서 양측 폐문림프절 비대가 확인되었다. 기관지 내시경을 이용한 조직검사상 비건락성 육아종성 염증이 관찰되었으며 항산균 염색은 음성이었다. 이에 사르코이드증 진단하 경정맥 고용량 메틸프레드니솔론 투여 후 경구 프레드니솔론을 6개월간 서서히 감량하며 투여하여 좌안 시력은 호전되었다.
결론
사르코이드증과 관련된 증상으로 시신경주위염이 발생할 수 있으며, 다른 전신 증상이 나타나기 전 초기 증상으로 발현할 수 있으므로 감별이 필요하다.
Trans Abstract
Purpose
To report a rare case of optic perineuritis as the presenting sign of sarcoidosis.
Case summary
A 57-year-old man presented with decreased visual acuity and pain with extraocular movement in his left eye starting 2 weeks earlier. He had a history of asymptomatic optic perineuritis in that eye 18 months previously, which had improved after 1 month on oral prednisolone. His best corrected visual acuity had decreased to 20/50 and he also had relative afferent pupillary defect and color vision defects in the left eye. Slit lamp examination results were normal. There were no inflammatory reactions in the anterior chamber or vitreous. Fundoscopy showed optic disc edema. Orbital magnetic resonance imaging showed diffuse enhancement surrounding the left optic nerve. The serum levels of eosinophil cationic protein and angiotensin- converting enzyme were markedly increased. A chest radiograph showed bilateral hilar lymph node enlargement. A biopsy via endobronchial ultrasound-guided transbronchial needle aspiration revealed multifocal non-caseating granulomas. Acid fast bacilli stain showed no evidence of tuberculosis. Based on these findings, he was diagnosed with sarcoidosis. After treatment with high-dose intravenous methylprednisolone and subsequent tapering with oral prednisolone for 6 months, the visual acuity improved.
Conclusions
Optic perineuritis can be the initial sign of sarcoidosis. Therefore, sarcoidosis should be considered in the differential diagnosis of optic perineuritis.
사르코이드증은 전신을 침범하는 비건락성 육아종이 특징인 질환으로 일반적으로 만 50세 이전에 발병하며, 남성과 여성이 비슷하거나 여성에서 조금 더 흔히 발생하고, 아프리카계 미국인과 북유럽인의 유병률이 특히 높다[1-3]. 한국인에서 사르코이드증의 유병률은 10만 명 당 9.37명이고 평균 발생 나이는 53.2세이다[4]. 한편, 국내 사르코이드증의 연간 누적 발생률은 2011년 1,000만 명 당 70.91명에서 2015년 101.86명으로 점차 증가하고 있는 추세이다[5].
사르코이드증은 흔히 폐 또는 종격동 림프절을 침범하며 이외에도 안구 및 눈부속기관, 말초 림프절, 피부, 중추신경계, 심장 등 전신을 침범한다[1]. 사르코이드증의 가장 흔한 눈 합병증은 포도막염이며 결막을 침범하는 경우 결막결절이나 결막염이 생길 수 있다[6]. 안와 및 눈부속기관 중에서는 눈물샘을 흔히 침범하며 눈꺼풀, 외안근, 안와지방, 혹은 시신경집을 침범하기도 한다[6]. 사르코이드증이 시신경과 시각경로를 침범할 경우 시력감소나 시야장애를 야기할 수 있으며 안면신경을 침범하면 노출각막병증, 눈물흘림, 눈꺼풀겉말림 등이 발생한다[6].
이 증례는 우연히 발견된 단안 시신경유두부종을 주소로 내원한 57세 남자에서 시신경주위염을 확인하고 이후 염증이 재발하여 조직검사 및 전신검사를 통해 사르코이드증을 진단하고 치료하였다. 사르코이드증은 안구와 안구 주변을 침범할 수 있으나 다른 전신 증상 없이 시신경주위염이 사르코이드증의 첫 발현 징후로 나타난 사례는 국내에서 보고된 바가 없어 소개하고자 한다.
증례보고
57세 남자가 안구건조증으로 인근 안과를 방문하였다가 우연히 좌안 시신경유두부종이 발견되었다. 환자는 좌측 주시시 회전성 어지럼증이 있었으나 주관적인 시력저하는 없었으며 좌안에 끈적거리는 느낌의 불편감과 양안 안구건조증만을 호소하였다. 과거력에서 혈압이나 당뇨 등 기저질환은 없었으며 가족력이나 외상, 수술, 약물 복용력은 특이 사항이 없었다.
교정시력은 우안 20/20, 좌안 20/20이었고, 사시각검사에서 원거리 및 근거리 모두 정위였고, 세극등현미경검사에서 양안 경도의 백내장 외 특이 소견은 없었으며, 안구돌출계검사에서 양안 모두 14 mm로 차이가 없었다. H-R-R 색각검사에서 양안 정상이었고, 대광반사는 좌안이 우안에 비하여 감소해 있었으며, 좌안 상대구심동공운동장애가 관찰되었다. 안저검사에서 좌안 시신경유두부종이 관찰되었으며(Fig. 1A), 빛간섭단층촬영에서는 좌안 상비측 시신경유두주변 망막신경섬유층 두께가 정상에 비해 증가한 소견이 보였다(Fig. 1B). 험프리시야검사(Humphrey Field Analyzer, Carl Zeiss Meditec, Dublin, CA, USA; 24-2 SITA-standard)에서 좌안에 비특이적인 시야협착이 관찰되었다. 혈액검사에서 당화혈색소, 전혈구검사는 정상 수치였으며, 혈청검사에서 매독균, B형간염바이러스, C형간염바이러스, 인체면역결핍바이러스, 톡소플라즈마 감염 소견은 없었고 안지오텐신전환효소(angiotensin-converting enzyme)는 39.1 U/L로 정상 범위였다. 또한 흉부방사선검사에서 특이 소견은 없었다(Fig. 2A). Gadolinium 조영제를 사용한 안와자기공명영상에서 좌측 시신경주위 앞부분 및 공막 경계부를 따라 경계가 불분명한 조영증강이 확인되었으며 시신경교차 전좌측 시신경 두께가 증가하였다(Fig. 3A). 이에 좌측 시신경주위염 진단 후 경구 프레드니솔론(Prednisolone, Solondo®; Yuhan Medical Corp., Seoul, Korea)을 하루 40 mg 7일, 30 mg 7일 투여하였다. 치료 1개월 후 좌안의 시신경부종은 감소하였다. 이후 환자가 내원하지 않아 추적 관찰이 중단되었다.

Fundus photographs and optical coherence tomography findings at the initial visit, revisitation after 1.5 years, and after steroid treatment. (A) At initial presentation, optic disc edema was prominent in the left eye (OS). (B) There was mild swelling of the superonasal circumpapillary retinal nerve fiber layer (RNFL) OS at the initial visit. (C) After 1.5 years, left optic disc edema had recurred. (D) Subretinal fluid and cystoid macular edema OS were also seen at revisitation. (E) After treatment with systemic steroids, optic disc edema had resolved leaving temporal pallor. (F) Diffuse RNFL thinning OS was observed after treatment.
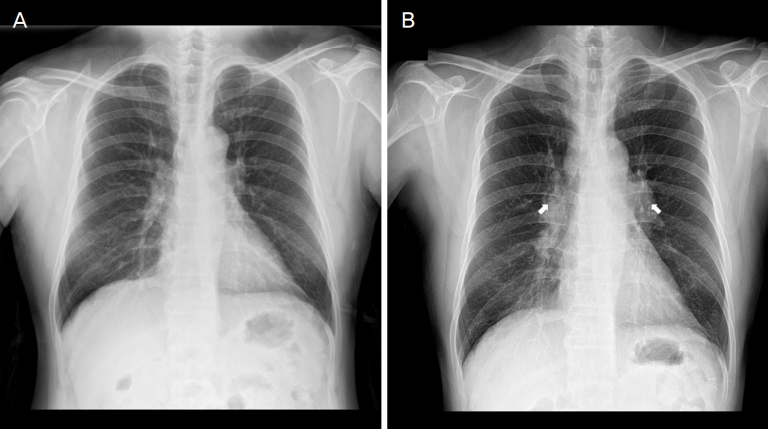
Chest radiographs at the intial and follow-up examination after 1.5 years. (A) At initial visit, there was no active lesion in both lungs. (B) After 1.5 years, multiple homogenous, symmetric lymph node enlargements (arrows) were seen at the right lower neck, mediastinal, both hilar and interlobar areas.
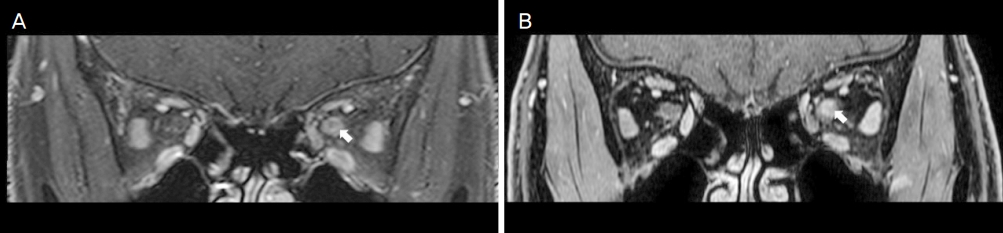
Orbital magnetic resonance imaging at the initial and follow-up examination after 1.5 years. (A) At the initial visit, ill-defined contrast enhancement (arrow) surrounding the anterior portion of the left optic nerve was seen on T1-weighted contrast-enhanced coronal image. (B) After 1.5 years, diffuse circumferential enhancement (arrow) of the intraorbital segment of the left optic nerve was seen on T1-weighted contrast-enhanced coronal image.
1년 6개월 뒤, 환자는 2주 전에 갑자기 발생한 좌안 시력 저하를 주소로 다시 내원하였다. 그동안 양안 앞포도막염이 여러 차례 발생하여 일차의료기관에서 치료받은 병력이 있었다. 최대교정시력은 우안 20/20, 좌안 20/50이었으며 눈운동 시 좌안 통증을 호소하였다. H-R-R 색각검사에서 우안 정상이었고 좌안은 선별검사판을 식별하지 못하였다. 좌안 상대구심동공운동장애가 관찰되었고, 세극등현미경검사에서 전방과 유리체에 염증세포 등 특이 소견은 없었다. 안저 사진에서 좌안 시신경부종 소견이 확인되었고(Fig. 1C) 빛간섭단층촬영에서 좌안 황반부 망막하액이 관찰되었다(Fig. 1D). 험프리시야검사에서 좌안 전체 시야결손(mean deviation -31.93 dB)이 확인되었다. 혈액검사에서 호산구양이온단백(eosinophil cationic protein)은 34.1 ng/mL, 안지오텐신전환효소는 83.5 U/L로 상승하였다. 형광안저혈관조영술에서 혈관 주변 누출은 없었다. 안와자기공명영상에서 좌측 시신경의 미만성 부종과 주위의 조영증강 소견이 있었다(Fig. 3B). 이학적 검사 및 병력청취에서 30대 이후 재발하는 정강이 골수염 및 족저근막염이 있었으며 두피와 허벅지에 재발성 궤양성 병변이 있었다. 구강 및 성기궤양은 부인하였다. 흉부 방사선검사에서 이전에 비해 양측 폐문림프절이 비대하였다(Fig. 2B). 이에 결핵 림프절염 혹은 사르코이드증 가능성을 고려하여 폐문림프절에 대해 기관지 내시경을 이용한 생검을 시행하였다.
조직병리검사에서 상피 모양 조직구로 이루어진 비건락성육아종성 염증이 관찰되었으며(Fig. 4), 악성 세포는 관찰되지 않았고, 항산성 염색(acid-fast bacilli stain, AFB)은 음성이었다. 이에 사르코이드증에 의한 좌안 시신경주위염 진단 후 5일간 정맥 주사로 메틸프레드니솔론(Methylprednisolone, Salon®; Hanlim pharmaceuticals, Seoul, Korea)을 하루 1 g 투여하였다. 치료 5일째 좌안 교정시력이 20/30으로 회복되었으며, H-R-R 색각검사에서 좌안에 경도의 적녹 색각이상, 강한 청황 색각이상이 확인되었다. 이후 6개월간 경구프레드니솔론(Prednisolone, Solondo®; Yuhan Medical Corp., Seoul, Korea)을 하루 60 mg 2주, 30 mg 1개월, 20 mg 1개월, 15 mg 2개월, 10 mg 2개월로 점차 감량하며 투여 후 중단하였다. 치료 6개월 후 좌안의 시신경부종은 호전되었고(Fig. 1E), 빛간섭단층촬영에서 좌안에 광범위한 시신경유두주위 망막신경섬유층의 위축이 확인되었다(Fig. 1F). 험프리시야검사에서 좌안 시야결손은 부분적으로 호전되었다. 좌안 교정시력은 20/25까지 회복되었으며 스테로이드 중단 후 4개월까지 재발 없이 유지되고 있다.

Photomicrographs of the lymph node biopsy harvested by endobronchial ultrasound-guided transbronchial needle aspiration. (A) Multiple well formed, non-caseating granulomas (arrows) (hematoxylin and eosin [H&E] stain, ×40). (B) A non-caseating granuloma (H&E, ×200). (C) A granuloma composed predominantly of epithelioid histiocytes (H&E stain, ×400). Special stains for acid fast bacteria and fungi (Ziehl-Neelsen and Periodic acid-Schiff-diastase, not shown) were negative for infectious organisms.
고 찰
이 증례는 다른 전신 증상 없이 단안의 시신경유두부종과 시신경주위염이 사르코이드증의 첫 발현 징후로 나타난 국내 첫 증례보고이다. 이 증례에서는 다른 신경학적 증상이나 호흡기 증상 등을 동반하지 않으면서 단안에 시신경 주위염이 반복적으로 발생한 환자에서 재발하는 궤양성 피부 병변에 대한 병력청취, 염증질환을 감별하기 위한 혈청 안지오텐신전환효소 상승 확인, 흉부 방사선검사에서 폐문 및 종격동 림프절 비대, 기관지 내시경을 통한 조직 채취 및 병리검사, 결핵과 진균 감염을 배제하기 위한 AFB, 메테나민은염색(methenamine silver stain), periodic acid-Schiff stain, 인터페론감마분비검사 등 다양한 보조검사를 통해 사르코이드증을 진단하고 치료하였다.
아직까지 사르코이드증을 확진하는 방법은 없다. 특징적인 비건락성 육아종이 병리조직학적으로 확인되면 임상 소견을 통해 비건락성 육아종을 형성할 수 있는 다른 질환을 배제해야 한다. 결핵, 매독, 톡소플라즈마증, 헤르페스바이러스 감염증, 아데노바이러스 감염증, 라임병, 사람T세포림프친화바이러스 1형 감염증, 칸디다증, 클라미디아 감염증, 전염성 연속종 등 다양한 감염질환을 배제해야 하며, 다발경화증, 쇼그렌증후군, 그레이브스병, 보그트-고야나기-하라다 증후군, 반응성 림프절 증식증, 안와 가성종양과 같은 염증질환도 감별해야 한다[7]. 또한 림프종이나 다른 원발 종양 전이나 침윤을 감별해야 하며, 영양 결핍 혹은 독성 물질에 의한 반응 여부를 확인해야 하겠다[7].
사르코이드증 치료는 스테로이드 투여가 일반적이며, 아직까지 가장 적합한 용량과 지속 기간에 대한 무작위 전향적 연구는 시행된 바 없어 개인별 맞춤 치료가 필요하다. 일반적으로 매일 경구 Prednisone 20-40 mg을 1개월에서 3개월간 유지한 후 반응이 있으면 하루 5-10 mg으로 감량하여 총 6개월 이상 복용 기간을 유지하는 것이 추천된다[8]. 국소 안구 병변의 경우 안구 주위에 스테로이드를 주사하기도 한다[9]. 급성 혹은 아급성 사르코이드증은 스테로이드 치료에 빠르게 반응하며, 만성 사르코이드증에서는 스테로이드에 반응하지 않기도 한다[10]. 스테로이드가 효과가 없거나 부작용이 있는 경우에는 세포독성제제, 항종양괴사인자제제 등이 대체제로 쓰일 수 있다[8].
사르코이드증의 5-10% 정도는 신경학적 침범을 하며, 주로 뇌신경병증을 일으킨다[11]. 시신경은 안면신경에 이어 두번째로 흔히 침범되는 뇌신경으로 전체 사르코이드증의 1-5% 정도에서 시신경을 침범한다고 알려져 있다[11,12]. 그러나 다른 중추신경계 침범의 징후 없이 시신경을 침범하는 경우는 드물다[12]. Koczman et al [13]은 신경사르코이드증으로 진단된 20명 중 14명(70%)에서 시신경이 침범되어 주로 시신경유두부종 및 시력저하로 증상이 발현되었으며, 안와자기공명영상에서 시각 경로의 병적인 조영증강이 흔히 관찰되었고, 스테로이드 치료 후에도 시신경 조영증강이 지속되면 예후가 나빴다고 보고하였다. Suresh et al [12]은 시신경에 한정되어 침범한 사르코이드증 환자 3명에서 시신경 조직검사를 시행하여 비건락성 육아종을 확인하였으며, 이처럼 전신 침범이 없는 경우 시신경수막종이나 교종, 혹은 다른 시신경병증을 감별해야 한다고 강조하였다. Kidd et al [14]은 중심시력저하 및 색각저하, 시야장애, 동공반응이상으로 발현한 사르코이드증 관련 시신경병증 환자 52명을 조사하여 시신경염과 유사한 아급성 시신경병증군과 서서히 진행하는 시신경병증군으로 분류하였으며, 통증은 27%에서만 동반되었고, 31%에서 양안을 침범하였으며, 진행성 시신경병증의 경우 스테로이드를 더 고용량으로 장기간 사용하더라도 예후가 나쁘다는 것을 확인하였다.
결론으로 사르코이드증은 매우 드물고 증상 또한 비특이적인 질환으로, 침범하는 부위에 따라 다양한 안과적 합병증을 유발할 수 있다. 이 증례와 같이 사르코이드증이 시신경과 주위조직을 침범하여 염증을 일으킬 경우 초기 증상으로 시력저하와 안구운동 시 통증이 나타날 수 있고, 진단 및 치료 시기를 놓칠 경우 시신경손상으로 인한 비가역적인 시력 및 시야장애를 일으킬 수 있다. 또한 사르코이드증이 눈에만 국한되지 않고 주요 장기를 침범할 경우 드물게 만성 섬유화가 진행되어, 적극적인 치료에도 불구하고 사망에 이를 수 있으므로 다른 전신 증상이 나타나기 전 시신경주위염이 초기 증상으로 나타날 수 있다는 점을 인지하고 조기에 감별하는 것이 중요하다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
노유진 / Yu Jin Roh
서울대학교 의과대학 분당서울대학교병원 안과학교실
Department of Ophthalmology, Seoul National University Bundang Hospital, Seoul National University College of Medicine
