중뇌주변부 뇌조의 지주막하출혈로 인한 시각로 손상
Optic Tract Injury Caused by Subarachnoid Hemorrhage in Perimesencephalic Cistern
Article information
Abstract
목적
시각로의 병변은 영상에서 미세한 변화만을 일으켜 놓치는 경우가 종종 보고되므로 세심한 관찰이 요구된다. 저자들은 중뇌주변부 뇌조의 지주막하출혈에 동반된 시각로 손상 1예를 경험하고 이를 보고하고자 한다.
증례요약
26세 여자 환자가 1개월 전부터 인지한 우측 시야가 불편하다는 증상을 주소로 내원하였다. 과거력상 40일 전 교통사고로 인한 양측 전두엽의 외상성 경막하출혈로 입원 치료를 받았으며 퇴원 후 우측 시야장애를 인지하고 안과로 내원하였다. 시력은 양안 1.0이며 우안에 구심동공운동장애가 있었다. 시야검사상 우측의 동명성 반맹이 있었고, 빛간섭단층촬영상 양안에서 좌측 황반부 신경절세포-내망상층의 두께가 얇아진 소견이 관찰되어 좌측 시각로의 병변을 의심하였다. 자기공명영상의 T2 강조영상에서 전두엽의 경막하출혈 외에는 시각 경로에 이상 소견이 발견되지 않았으나, 자화강조영상에서 왼쪽 중뇌주변부 뇌조에 미세한 지주막하출혈이 관찰되었으며 이로 인한 시각로의 손상으로 진단할 수 있었다.
결론
저자들은 좌측 시각로 손상이 의심되는 26세 여자 환자에서 자기공명영상의 자화강조영상에서 중뇌주변부 뇌조의 지주막하출혈을 확인하고 이를 보고하는 바이다.
Trans Abstract
Purpose
A case of optic tract injury caused by subarachnoid hemorrhage in the perimesencephalic cistern is reported.
Case summary
A 26-year-old female with a history of traumatic subdural hemorrhage along the bilateral frontal convexity presented with a right visual field defect. Her visual acuity was 1.0 in both eyes. Slit-lamp examination and fundus examination were not remarkable. There was a relative afferent pupillary defect in the right eye. A Humphrey visual field test revealed right homonymous hemianopsia. Optical coherence tomography showed left homonymous hemiatrophy of the ganglion cell-inner plexiform layer in both eyes. Magnetic resonance imaging was performed. Susceptibility-weighted images showed minimal subarachnoid hemorrhage in the left perimesencephalic cistern, and the patient was confirmed to have optic tract injury due to subarachnoid hemorrhage.
Conclusions
We report a case of optic tract injury in a 26-year-old patient caused by subarachnoid hemorrhage in the perimesencephalic cistern, which was confirmed by susceptibility-weighted images.
시각로(optic tract)는 시각교차부터 가쪽무릎체(lateral geniculate body)까지를 연결하는 신경섬유다발이다. 시각로의 병변은 특징적인 임상양상을 보이며, 반대쪽 눈의 구심동공운동장애, 반대쪽 동명성 반맹과 안저검사상 반대쪽 눈의 띠 형태의 시신경유두위축(bowtie atrophy)을 관찰할 수 있다. 빛간섭단층촬영검사에서는 양안에서 병변과 같은쪽 절반의 황반부 신경절세포-내망상(ganglion cell-inner plexiform layer)의 두께가 얇아진다[1,2]. 뇌의 자기공명영상을 통해 시각로의 병변을 확진할 수 있으나, 시각로는 비교적 얇은 구조로 이루어져 있고, 영상에서 미세한 변화만을 일으켜 이를 간과하고 놓치는 경우가 종종 보고된다[3]. 저자들은 중뇌주변부 뇌조(perimesencephalic cistern)의 지주막하출혈에 동반된 시각로 손상 1예를 경험하여 이를 보고하고자 한다.
증례보고
특이 전신질환이 없는 26세 여자 환자가 1개월 전부터 인지한 우측 시야가 불편하다는 증상을 주소로 내원하였다. 과거력상 40일 전 교통사고로 인한 양측 전두엽의 외상성 경막하출혈로 입원치료를 받은 적 있으며, 퇴원 후 우측 시야장애를 인지하였다.
내원 시 시력은 양안 1.0이었으며, 안압은 양안 18 mmHg이었다. 세극등을 이용한 전안부검사상 특이 소견은 없었으며, 우안에 구심동공운동장애가 있었다. 안저검사상 뚜렷한 시신경위축은 보이지 않았다. 험프리 자동시야검사상 오른쪽 동명성 반맹이 있었고, 빛간섭단층촬영검사상 양안에서 좌측 절반 황반부 신경절세포-내망상층의 두께가 얇아진 소견이 관찰되었다(Fig. 1, 2). 좌측 시각로의 병변을 의심하여 자기공명영상을 촬영하였으며, T2 강조영상(T2-weighted image)에서 전두엽의 경막하출혈 외에는 시각 경로(visual pathway)에 이상 소견이 발견되지 않았으나, 자화강조영상(susceptibility-weighted image)에서 왼쪽 중뇌 주변부 뇌조에 미세한 지주막하출혈이 관찰되어, 이로 인한 시각로의 손상으로 진단하였다(Fig. 3). 외상 후 8개월째 내원 시 시야검사상 동명성 반맹의 범위는 다소 줄어들었으나, 안저 소견과 빛간섭단층촬영 소견은 변화가 없었다. 후속 자기공명영상에서 좌측 시각로가 우측에 비해 얇아져 시각로 위축이 진행하였음을 알 수 있었다(Fig. 4).

Humphrey Visual field test at presentation. Visual field test shows right homonymous hemianopsia.
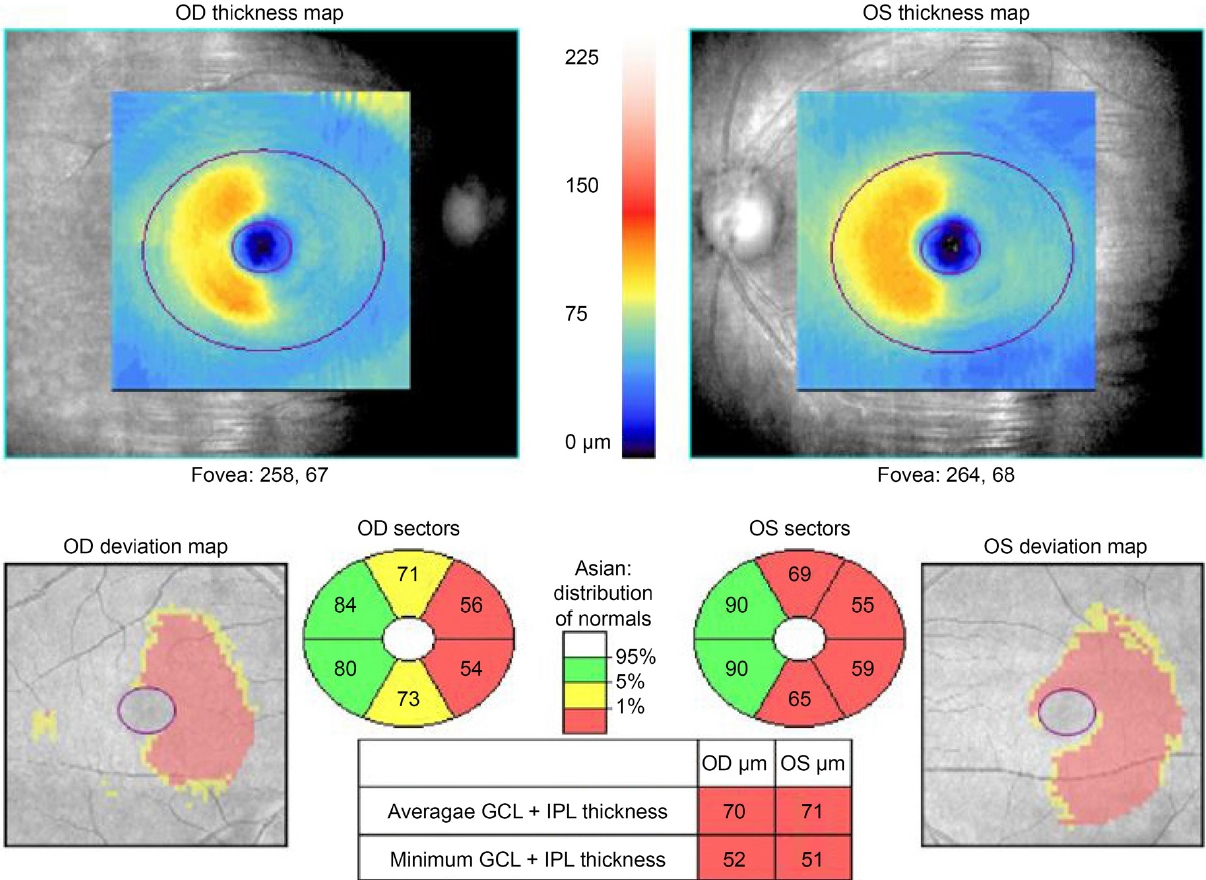
Ganglion cell analysis of optical coherence tomography at presentation. Ganglion cell-inner plexiform layer scan shows left hemiatrophy in both eyes. OD=oculus dexter; OS=oculus sinister; GCL=ganglion cell layer; IPL=inner plexiform layer.

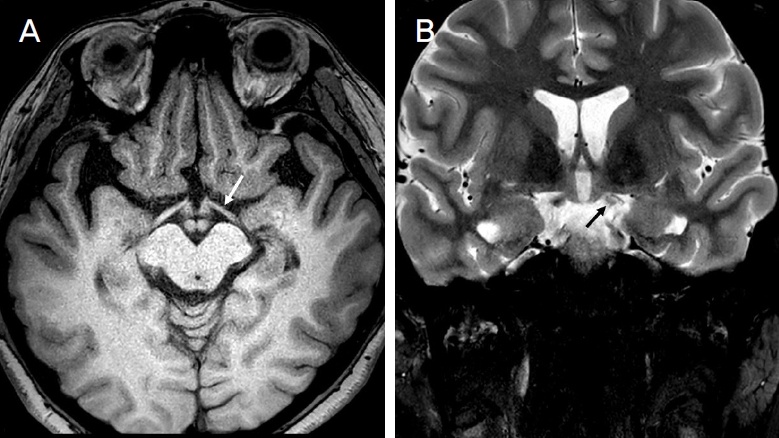
Magnetic resonance image at presentation. (A) T2-weighted image shows no definite abnormality along the visual pathway. (B) Susceptibility-weighted image shows minute subarachnoid hemorrhage in the left perimesencephalic cistern (arrow).
Magnetic resonance image eight months after the head trauma. (A) T1-weighted image shows mild thinning of optic tract (arrow). (B) T2-weighted image shows high signal intensity of left optic tract (arrow).
고 찰
시각로는 종양, 혈관 기형, 동맥류, 외상, 염증성 질환 등의 원인으로 인해 손상받을 수 있다[3]. 이러한 시각로의 병변은 반대쪽 동명성 반맹과 반대쪽 눈의 구심동공운동장애를 특징으로 한다. 해부학적으로 시각로는 병변과 같은 쪽 눈의 비측 시야를 담당하는 신경섬유보다 반대쪽 눈에서 교차하여 이측 시야를 담당하는 신경섬유를 더 많이 포함하고 있기 때문에 구심동공운동장애는 반대편 눈에 나타나게 된다. 또한, 신경절세포의 변화로 인해 빛간섭단층촬영에서 양안에 병변과 같은 쪽의 신경절세포-내망상층의 두께가 얇아지며, 축삭의 특징적인 주행 구조는 반대편 눈에 띠 형태의 시신경유두위축을 일으킨다[1,2].
이러한 특징적인 임상양상에도 불구하고, 시각로는 대뇌각(cerebral peduncle)과 전방 측두엽(anterior temporal lobe) 사이의 비교적 얇은 구조로 이루어져 있어, 영상검사에서 간과하고 놓치는 경우가 종종 있다. 또한 우리나라에서 시각로의 단독 병변은 단 3예가 보고되어 있으며[4-6], 뇌하수체졸중 환자에서 시교차와 시각로의 출혈 증례가 보고된 바 있다[7].
시각로 손상의 원인은 크게 주변부 구조에 의한 외인성 병변과 시각로 자체의 내인성 병변으로 구분할 수 있다. 외인성 손상은 측두엽, 중뇌, 기저핵(basal ganglia), 가쪽무릎체 및 안장위(suprasella) 등의 병변에 의해 시각로가 구조적으로 압박되는 경우로, 이는 영상에서 시각로가 눌리거나 전위되어 관찰된다[3]. 내인성 손상은 뇌경색이나 외상성 뇌손상 등에 의해 생길 수 있으며 영상검사에서 시각로 자체가 얇아지거나 두꺼워지는 소견이 보일 수 있는데, 이런 병변은 매우 미세하여 외인성 손상에 비해 놓치기 쉽다[3]. Kowal et al [3]은 환자들의 영상을 영상의학과 전문의에게 판독을 의뢰하였을 때 외인성 손상 24예 중 4예(16%)에서, 내인성 손상 15예 중 15예(100%)에서 시각로의 병변을 놓친 것을 보고한 바 있다.
한편, 빛간섭단층촬영이 시각로 병변의 진단에 유용할 수 있다. 망막신경섬유층의 두께 변화로 시각로의 병변을 진단할 수 있다는 논문도 있으나, 최근 한 논문에서 신경절세포-내망상층의 위축이 망막신경섬유층 두께 변화보다 시각로 병변의 진단에 민감도가 더 높다고 밝혔다[5,8]. 신경절세포-내망상층의 위축은 무릎체 뒤쪽(retrogeniculate) 병변에서도 역행성 시냅스 간 신경절세포 변성(retrograde transsynaptic degeneration)으로 인해 관찰될 수 있다. 그러나, 무릎체 앞쪽(pregeniculate) 병변에서는 1개월 이내에 나타나는 반면, 뒤쪽 병변은 약 5개월이 지나서 서서히 나타나기 때문에 이런 시간적인 특성을 바탕으로 시각로의 병변과 무릎체 뒤쪽 병변을 감별할 수 있다[8].
본 증례는 우안의 구심동공운동장애, 우측 동명성 반맹, 1달 이내의 양안의 좌측 신경절세포-내망상층의 두께 변화를 토대로 좌측 시각로 질환으로 의심하였다. 일반적으로 자기공명검사의 T2 강조영상은 출혈의 급성, 아급성, 만성 경과에 따라 신호강도가 다르게 나타나 뇌출혈을 감별하는데 유용하게 사용되는 영상이나, 본 증례에서는 주변 실질 및 출혈 부위가 모두 저신호강도를 보여 구별하기 어려웠다. 반면 탈산소혈액(deoxygenated blood)을 민감하게 구별할 수 있는 자화강조영상에서 좌측 중뇌주변부 뇌조에 저신호강도를 보이는 미세한 출혈을 확인할 수 있었고, 이에 출혈에 동반된 시각로 손상으로 확진할 수 있었다[9]. 결론적으로 저자들은 시각로 손상이 의심되는 환자에서 자기공명영상의 자화강조영상에서 중뇌주변부 뇌조의 지주막하출혈을 확인하였으며, 시각로 병변이 의심되는 경우 자기공명영상의 세심한 관찰이 필요할 것으로 생각하여 이를 보고하는 바이다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
이승재 / Seung Jae Lee
연세대학교 의과대학 안과학교실
Department of Ophthalmology, Yonsei University College of Medicine
