젊은 남성에서 발생한 Relentless Placoid Chorioretinitis
Relentless Placoid Chorioretinitis in a Young Man
Article information
Abstract
목적
16개월 동안 반복된 다발판모양 병변과 망막색소상피의 위축성 변화를 보인 relentless placoid chorioretinitis 증례를 보고하고자 한다.
증례요약
21세 남자가 시야 흐림을 주소로 내원하였다. 교정시력은 우안 20/50, 좌안 20/20였다. 안저에 다발판모양 백색 병변이 관찰되었으며, 전방염증 소견은 관찰되지 않았다. 실험실 검사상 감염의 증거는 없었다. 임상 추정 진단으로 급성후부다발판모양색소상피병증이나 비감염성 뒤포도막염으로 생각하고 경구 스테로이드 치료를 시행하였다. 7개월간 병변이 양안에서 반복적으로 발생하여 경구 스테로이드 및 면역억제제 치료를 시행하였고, 내원 16개월 후 재발 없이 양안 교정시력 20/20으로 유지하고 있다. 수십개의 망막색소상피의 위축 소견을 남겼으며 임상경과와 병변의 소견을 통해 relentless placoid chorioretinitis로 진단하였다.
결론
만성적인 다발판모양 백색 병변과 망막색소상피의 위축성 변화가 망막 중심 및 주변부까지 발생할 경우 relentless placoid chorioretinitis를 고려해야 하며, 시력개선을 위해 적극적인 면역억제제 치료가 필요하다.
Trans Abstract
Purpose
To report a patient with relentless placoid chorioretinitis who showed recurrent multiple placoid lesions and retinal pigment epithelial atrophic changes in both eyes for more than 16 months.
Case summary
A 21-year-old man visited our clinic because of visual disturbance in both eyes. The best-corrected visual acuities were 20/50 and 20/20 in the right and left eyes, respectively. The fundus showed multiple whitish placoid lesions from the posterior pole to the mid-periphery. There were no anterior chamber inflammation signs. To exclude systemic and infectious etiologies, laboratory workup was performed. All tests were negative except for the serological types HLAB13 and B51. Based on clinical estimation, we made a diagnosis of acute posterior multifocal placoid pigment epitheliopathy or posterior uveitis and prescribed oral methylprednisolone for the patient. However, multiple white dot lesions occurred repeatedly in both eyes for 7 months. With the oral methylprednisolone and immunosuppressive treatment, the best-corrected visual acuity of both eyes was maintained at 20/20 without further recurrence 16 months after the first visit. The lesions left atrophic findings in the retinal pigment epithelium. We diagnosed the patient with relentless placoid chorioretinitis, based on the prolonged clinical course and widespread lesion distribution.
Conclusions
Relentless placoid chorioretinitis should be considered in patients with chronically progressive multiple white dot lesions and retinal pigment epithelium atrophic changes between the central pole and the periphery. Aggressive immunosuppressive treatment should be performed to improve the patient's visual outcome.
Relentless placoid chorioretinitis는 급성후부다발판모양 색소상피병증(acute posterior multifocal placoid pigment epitheliopathy, APMPPE), 뱀모양맥락막염(serpiginous choroiditis, SPC)과 유사한 질환이다. 하지만 이들과는 달리 광범위한 병변의 분포, 경과의 만성화, 50개 이상의 병변 등 비전형적인 임상양상을 보이는 매우 드문 질환으로 알려져있다[1,2]. Relentless placoid chorioretinitis는 2000년 Jones et al [1]이 임상적 질환군으로 처음 명명하였고 동양에서는 2005년 일본의 Orihara et al, [3] 2019년 Asano et al [4]이 젊은 남성에서 발생한 사례 및 adalimumab을 이용해 치료한 사례를 보고한 바 있다. 현재까지 국내에서는 relentless placoid chorioretinitis의 임상양상 및 치료에 대한 보고가 없다. 저자들은 16개월 기간 동안 호전과 악화를 반복하며 만성적으로 진행하는 비전형적인 맥락망막염을 경험하고 치료를 하였고, 이 증례를 relentless placoid chorioretinitis으로 진단하였기에 이를 보고하고자 한다.
증례보고
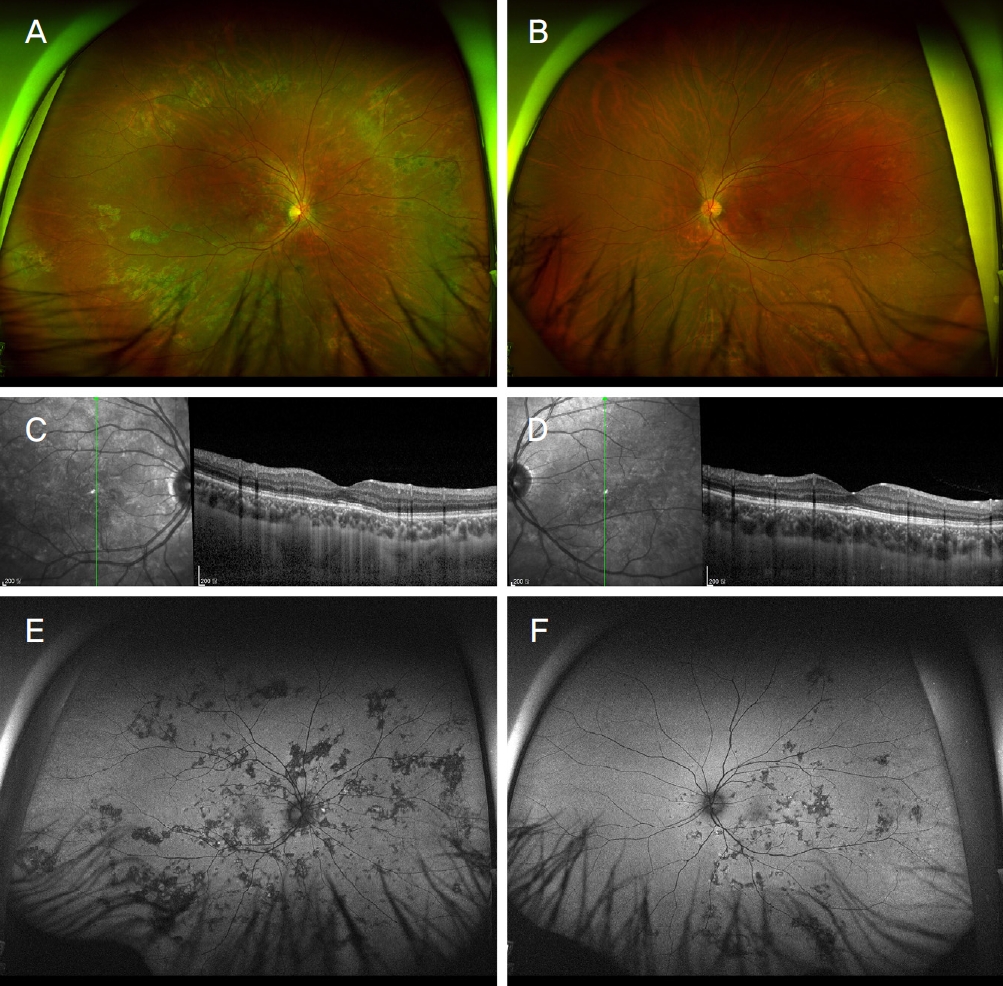
21세 남자 환자가 내원 2일 전부터 시작된 우안의 시력저하와 양안의 시야 장애를 주소로 내원하였다. 지역 병원 방문 후 우안의 다발맥락막염으로 의심 하에 전원되었다. 건강한 남성으로, 안과적 수술력, 전신적 특이사항 및 약물 복용의 과거력은 없었다. 내원 당시 교정시력은 우안 20/50, 좌안 20/20, 안압은 우안 18 mmHg, 좌안 16 mmHg였다. 세극등현미경검사에서 전방염증은 관찰되지 않았고, 후방의 염증은 양안에서 1+ 관찰되었다. 안저검사상 다수의 황백색 판모양병변들이 양안 망막의 후극과 적도 주변에서 관찰되었다(Fig. 1A, B). 안저자가형광에서 급성 병변은 과형광으로, 망막색소상피가 소실된 외망막층은 저형광으로 관찰되었다(Fig. 1C, D). 빛간섭단층촬영(spectral domain optical coherence tomography)에서 광수용체층 내분절(photoreceptor layer inner segment)과 외분절(outer segment)의 경계 및 망막색소상피의 소실과 맥락막모세혈관층(lamina choriocapillaris)에서 다수의 고반사 결절이 관찰되었다(Fig. 1E, F). 형광안저혈관조영술에서 황반부의 불규칙한 초기 저형광소견, 후기 과형광 소견을 보였다. 인도사이아닌그린혈관조영술에서 초기 저형광 소견, 후기 저형광 소견을 보이며 시간이 지남에 따라 급성 병변의 경계가 더 뚜렷해짐을 관찰할 수 있었다(Fig. 1G-J). 주변부 형광안저혈관조영술에서 저형광 소견을 보이는 병변은 보이지 않았다(Fig. 1K, L). 감염의 원인을 비롯한 전신 인자를 배제하기 위해 전혈구 검사, 적혈구침강속도(erythrocyte sedimentation rate), C-반응단백(C-reactive protein), venereal disease research laboratory, human immunodeficiency virus, anti-Toxoplasma Ab, tuberculosis, 흉부 방사선검사 등이 시행되었으며 모두 음성으로 판명되었다. 또한 herpes simplex virus, varicella zoster virus, cytomegalovirus의 immunoglobulin G (IgG) 항체양성, IgM 항체는 모두 음성으로 급성 감염을 배제할 수 있었다. 한편, human leukocyte antigen (HLA)-B형에 대한 검사에서 B13과 B51 양성이었으나 류마티스 내과 협진에서 베체트병(Behcet’s disease)을 시사하는 전신 신체 소견을 보이지 않아, 임상적 의미를 보이지 않는다는 보고를 받았다.

Fundus photographs of both eyes upon initial examination. (A, B) Whitish lesions in the macula. Fundus autofluorescence images. Hypo and hyperfluorescence lesions in the right eye. (C) No lesion in the left eye. (D) Optical coherence tomography of both eyes. (E) Focal retinal pigment epithelium nodularity, disruption of the external limiting membrane, and loss of the photoreceptor inner segment/outer segment band in the right eye. (F) No focal outer retinal disruption in the left eye. Fluorescein angiography and indocyanine green angiography. (G, H) Hypofluorescence of the lesions in the early phase. (I, J) Fluorescein angiography showing hyperfluorescence of the lesions and indocyanine green angiography showing hypofluorescence of the lesions in the late phase. (K, L) Fluorescein angiography showing no lesions at the periphery and the equator.
환자를 통한 문진 및 임상 소견으로 보아 APMPPE와 뒤포도막염이 의심되었으며 경구 스테로이드(methylprednisolone 50 mg/day)를 7일간 처방하였다. 1주 뒤 망막 후극의 병변이 소실되는 양상을 보였다. 여드름 등의 피부 부작용 발생, 체중 증가, 얼굴의 화끈거림 등의 증상을 호소하여 3일 간격으로 10 mg씩 단계적으로 용량을 감량하였다. 4주 후 안저에서 관찰되던 판모양 백색 병변의 수가 현저히 감소하였다. 경구 스테로이드 치료 중단 후 2개월째, 최대교정시력 우안 20/50, 좌안 20/40으로 양안 시력저하를 호소하며 내원하였다. 세극등현미경검사에서 유리체염과 함께 망막후극과 적도 및 적도부 앞에 다수의 백색 병변과 망막색소상피의 위축성 변화가 새롭게 관찰되었다. 경구 스테로이드(methylprednisolone 80 mg/day)를 증량하여 경구 아자티오프린(azathioprine 150 mg/day)과 병용 투여하였다. 7개월간의 경과 관찰 기간 동안 아자티오프린의 용량은 일정하게 유지하며 경구 스테로이드는 일주일 간격으로 10 mg/day 씩 감량 후 4 mg/day으로 유지 치료를 하였다. 다수의 백색병변은 투여 7개월간의 경과 관찰 동안 호전과 악화를 반복하며 급성 병변과 만성 병변이 공존하는 모습을 보였다(Fig. 2). 병의 호전이 없는 것으로 판단하여 경구 스테로이드는 4 mg/day로 유지하며 아자티오프린을 메토트렉세이트(methotrexate 15 mg/week)로 교체하였다. 이후 새로운 병변의 출현이 감소하고 유리체염이 소실되었다. 모든 경구 치료약제는 감량하여 중단하였고 첫 내원 후 현재까지 16개월 동안 새로운 병변의 출현 없이 양안 최대 교정시력 20/20으로 유지되고 있으며, 병변이 있었던 영역은 망막색소상피의 위축성 변화를 남겼다(Fig. 3).

Fundus photographs of both eyes 7 months after the initial presentation. (A, B) Multiple lesions from the posterior pole to peripheral fundus. Fundus autofluorescence of both eyes 7 months after presentation. (C, D) Both hypo and hyperfluorescence lesions.
Fundus photographs of both eyes 1 year after the initial presentation. (A, B) More than 100 lesions with atrophic changes of the peripheral fundus lesions. Optical coherence tomography of both eyes 1 year after the presentation. (C, D) Alleviated focal outer retinal disruption and reduction of retinal thickness. Fundus autofluorescence of both eyes 1 year after the presentation. (E, F) Both hypo and hyperfluorescence lesions.
고 찰
본 증례는 건강한 젊은 남성에서 양안에 발생한 relentless placoid chorioretinitis 질환의 치료와 1년 이상의 임상 경과에 대한 보고이다. Relentless placoid chorioretinitis는 비감염성 포도막염인 APMPPE, SPC와 유사하나 비전형적인 임상양상을 보이는 드문 질환이다[1]. Relentless placoid chorioretinitis의 판모양 백색 병변은 APMPPE와 유사한 형태를 보인다[1]. 한편, 질병 후기에서 나타나는 맥락막위축의 모습은 SPC와 유사하다[1]. 본 증례는 후극과 유두부 주위를 주로 침범하는 SPC와 달리, 급성과 만성 병변이 혼재되어 적도 주변까지 침범된 양상을 보였다. APMPPE는 병변이 후극부에 국한되며, 수주 내에 자연 호전을 보이고 두통 등의 신경학적 증상을 동반할 수 있다. 반면, 본 증례는 수개월간의 전신 스테로이드 치료에도 불구하고 질병이 재발하였고, 적도 주변까지 병변이 침범하는 양상을 보였다.
Relentless placoid chorioretinitis는 일반적으로 중심 시야장애를 보이고, 급성의 무통성 시력저하가 두드러지며, 만성적 임상경과를 보인다[5]. 또한, 50개 이상 다수의 작은 병변들이 망막 후극부에서 적도 주변부까지 존재하며 맥락막과 망막색소상피층에 침윤된다[1]. 형광안저혈관조영술에서 병변이 초기 저형광과 후기 과형광되는 특징을 보인다. 빛간섭단층촬영검사에서 황반부의 망막하액, 망막색소상피층의 박리, 망막층의 고반사를 보이는 활동 병변을 관찰할 수 있다[2,3]. 본 증례에서도 만성적인 경과를 보이고, 양안에서 50개 이상의 병변이 관찰되었다. 형광안저혈관조영술은 동일한 소견을 관찰할 수 있었다. 그러나 본 증례는 기존 보고에서 언급된 빛간섭단층촬영 소견 중 망막층의 고반사만 관찰할 수 있었다.
Relentless placoid chorioretinitis는 병리학적으로 약 10여년 전부터 실체는 인지되었으나, 여전히 명백한 병인 및 소인은 밝혀지지 않았다[6]. 기존의 보고에 의하면, 환자들의 연령대는 17-51세, 성별의 차이는 보이지 않았다[1]. 또 다른 보고에 의하면 남성에서 더 흔히 발병되며, 발병 최소 연령은 34세였다[7].
본 증례는 포도막염이 동반되는 전신질환을 감별하기 위해 혈액검사를 시행하였으며, HLA-B형 검사에서 B13과 B51 양성을 보였다. 베체트병은 B5, B27, B51과 연관이 있다고 알려져 있다[8]. 베체트병과 관련된 안구 소견은 포도막염, 유리체염, 망막혈관염 등이 있으며 일반적으로 망막혈관염 양상이 많다. 맥락막두께가 증가하는 맥락막염을 보이는 경우도 보고되어 있다[9,10]. 본 사례의 경우 안저 소견을 통해 베체트병의 안구침범을 배제할 수 있었다. 그러나 혈액검사에서 B13과 B51의 양성을 보였기에 류마티스 내과협진을 의뢰하였다. 눈 증상을 제외한 구강 궤양, 성기 궤양, 결절 홍반 및 혈관염 등의 진단 기준을 만족하지 않아 위 질환을 배제할 수 있었다. 또한 감염질환에 대한 혈액검사가 음성을 보였고, 안저 소견을 통해 감염성 질환을 배제하였다.
Relentless placoid chorioretinitis는 다양한 치료 방법이 알려져 있으나 장기간의 치료 방법은 보고되지 않았으며, 일관된 치료 결과를 보이지 않았다[5]. Relentless placoid chorioretinitis 치료는 병변의 호전과 시력개선을 위해 전신스테로이드를 흔히 사용한다. 그러나 전신 스테로이드 용량을 점진적으로 줄이는 동안 재발하는 경향이 있다[1,11,12]. 항종양괴사인자(anti-tumor nercrosis factor) 약제인 adalimumab의 사용을 통해 면역억제제를 성공적으로 감량하였고 관찰 기간 동안 재발 없이 유지된 경우도 있었다[4]. 전신적인 스테로이드의 투여와 함께 cyclosporine, mycophenolate mofetil, 아자티오프린과 같은 다양한 면역억제제로 치료한 보고들이 있으나, 증례가 많지 않다[5,6]. 본 증례도 경구스테로이드(methylprednisolone 50 mg/day, 0.625 mg/kg)를 감량 후 중단하였을 때 재발하였다. 또한 경구 스테로이드 4 mg/day를 유지하며 아지티오프린(azathioprine 150 mg/day)을 병용하였으나 호전과 악화를 반복하였다. 반면 경구 스테로이드 4 mg/day를 유지하며 아지티오프린을 메토트렉세이트(methotrexate 15 mg/week)로 교체 후 염증이 안정적으로 조절되었다. Relentless placoid chorioretinitis의 치료에 대한 연구에서 전신 스테로이드 약제 내성에 대한 보고가 있었고, 질환의 재발을 제어하기 위한 면역억제제 추가가 필요하다는 보고가 있었다[1,2]. Cyclosporine 100-150 mg/day를 투여하며 재발 없이 전신적 corticosteroid의 점진적인 감소를 시행한 보고가 있었으며[1,6], 또 다른 보고에 의하면 mycophenolate mofetil 1,000-2,000 mg/day의 병용으로 15-18개월간의 재발이 없는 경우도 있었다[13,14].
Relentless placoid chorioretinitis 환자에서 메토트렉세이트를 이용한 치료는 보고된 바 없다. 본 증례 환자의 경우, 경구 메토트렉세이트와 경구 스테로이드 병합 요법을 통해 질환이 조절되었고, 경구 메토트렉세이트와 경구 스테로이드를 점진적으로 중단할 수 있었다. 현재 새로운 병변의 출현 없이 양안 최대교정시력 20/20으로 유지되고 있다. 결론적으로 안저검사에서 다발판모양 백색 병변과 망막색소상피의 위축성 변화가 중심부 및 주변부에서 만성적으로 진행하는 21세 남자 환자를 relentless placoid chorioretinitis로 진단하고 초기에 적극적인 스테로이드 치료와 함께 면역억제제의 추가적인 병합요법으로 좋은 시력예후를 보였기에 이를 보고하고자 한다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
김태훈 / Tae Hoon Kim
고신대학교 의과대학 안과학교실
Department of Ophthalmology, Kosin University College of Medicine
