2016년도 국민건강영양조사를 바탕으로 한 소아의 약시 유병률 조사
The 2016 Korea National Health and Nutritional Examination Survey of the Prevalence of Amblyopia
Article information
Abstract
목적
2016년 국민건강영양조사를 바탕으로 5세에서 8세 소아의 약시 유병률을 알아보고자 하였다.
대상과 방법
2016년 실시된 국민건강영양조사의 안과 검사 결과를 바탕으로, 전체 표본 443명 중 시력을 측정한 420명을 분석하였다. 나안시력이 0.8 미만인 경우 자동굴절검사를 사용한 굴절검사를 실시하여 최대교정시력을 측정하였다. 약시의 기준은 0.8 또는 0.63 미만으로 설정하였다. 자동굴절검사를 바탕으로 양안 굴절이상 차이가 구면렌즈 1.5디옵터 이상이거나 난시 1.0디옵터 이상과 양안의 경우 난시 2.5디옵터, 원시 4.0디옵터 이상인 경우 약시를 유발할 수 있는 의미 있는 굴절이상으로 정의하였다. 소아의 지역, 부모의 소득 수준을 비교 분석하였다.
결과
전체 420명(남:여=219:201) 중 0.8 미만과 0.63을 기준으로 한 약시의 유병률은 각각 21명(5.0%)과 16명(3.8%)이었다. 연령별 약시 유병률(0.8 미만 기준)은 5세에서는 10명(10%), 6세 6명(5.6%), 7세 4명(3.8%), 8세 1명(0.9%)로 나이가 들수록 유병률이 줄어들었다. 의미 있는 굴절이상을 보인 경우가 전체 21명 중 9명(42.9%)이었다. 지역별 분포는 강원도, 충청남도에서 가장 높게 나타났으며 부모의 소득이 약시의 유병률에 영향을 미치지는 않았다(p=0.189).
결론
약시의 유병률은 나이가 들수록 줄어드는 양상을 보였으며 이는 약시를 조기에 발견하여 치료하는 것이 중요함을 의미한다. 따라서 약시를 조기에 발견할 수 있는 체계적인 안과검진이 중요할 것으로 생각된다.
Trans Abstract
Purpose
To investigate the prevalence of amblyopia in children between the ages of 5-8 years based on the Korean National Health and Nutrition Examination Survey (2016).
Methods
Based on the results of the Korean National Health and Nutrition Examination Survey conducted in 2016, among a total of 443 children, we measured and analyzed the visual acuities of 420 children. The visual acuity was measured using a conventional visual acuity chart. When the uncorrected visual acuity was < 0.8 in the first visual acuity test, a refraction test was performed using the automatic refraction test (KR-8800, Topcon, Tokyo, Japan) and the corrected visual acuity was measured. Unilateral amblyopia and bilateral amblyopia were defined as a ≥ 2 line difference between two eyes and visual acuity in the better eye < 0.8 or < 0.63. The significant refractive errors were defined as follows: the spherical lens was 1.5 diopters (D) or more, astigmatism was 1.0 D or more, or astigmatism of 2.5 D was 4.0 D or more.
Results
The prevalence of amblyopia was 5.0% (21 patients, < 0.8 in the better eye) and 3.8% (16 patients, < 0.63 in the better eye) in a total of 420 patients (male:female = 219:201). The prevalence of amblyopia in different age groups was: 10 (10%) at 5 years of age, 6 (5.6%) at 6 years of age, 3.8% at 7 years of age, and 0.9% at 8 years of age. Nine out of 21 patients (42.9%) had significant refractive errors. The regional distribution was highest in Gangwon-do and Chungcheongnam-do provinces and parental income did not affect the prevalence of amblyopia (p = 0.189).
Conclusions
The prevalence of amblyopia decreased with age suggesting that early detection and treatment of amblyopia are important. Therefore, systematic eye examinations that can detect amblyopia in the early stage may be important in the National Health Care results.
약시는 눈에 대한 신체진단검사에서 특별한 기질적 원인 없이 굴절이상을 교정한 후 한 눈의 시력이 스넬렌시력표상 2줄 이상 차이 나거나 두 눈의 시력이 정상보다 저하되어 있는 상태를 말한다. 전 인구의 2-5%에서 발견될 정도로 유병률이 낮지 않은 중요한 공중보건 질환이다[1-3]. 소아 감각기능의 발달 특성상 7-9세의 결정적 시기가 지나면 시각경로 신경계가 이미 고정 확립되어 약시치료의 성공률이 떨어진다[4]. 또한 20세 이상 성인에서 안과 검사상 발견되는한 눈 시력상실의 가장 큰 원인이 소아기 약시일 정도로 시력저하의 주요 원인으로 자리 잡고 있다[5].
약시는 조기에 발견하여 치료할수록 치료 효과가 좋으며 여러 국가에서 영유아건강검진에 시각검진이 포함되어 있다[6]. 국내에서도 국가에서 시행하는 영유아건강검진, 한국실명예방재단에서 시행하는 자가시력검진도구를 이용한 자가검진이 실시되고 있다. Lim et al [7]은 2004년 실명예방재단 자가검진도구를 이용한 약시 유병률 조사에서 약시의 유병률이 0.4%라고 보고하였으나 이는 서울에 거주하는 3-5세 소아만을 대상으로 하여 대한민국의 약시 유병률을 대표하기 어렵다. 따라서 약시에 대한 장기적인 정책을 수립하고 활동지표를 설정하기 위해 국민건강영양조사를 바탕으로 약시 유병률과 양상을 알아보고자 하였다.
대상과 방법
2016년 실시된 국민건강영양조사를 통해 취합된 자료를 바탕으로 분석하였으며 원시 자료를 이용한 본 연구는 헬싱키선언 준수 및 김안과병원 연구윤리심의위원회의 심의를 면제받았다(승인 번호: 2019-07-009). 국민건강영양조사에서는 연도에 따라 시력측정대상이 다르며 제7기 1차년도(2016)에는 만 5-19세를 대상으로 시력 및 굴절검사를 실시하였고, 제7기 2차년도(2017)는 만 40세 이상 80세까지 시력 및 굴절검사를 시행하였다. 본 연구는 5-8세 소아의 약시 유병률을 알아보고자 전체 443명 중 시력을 측정한 420명을 대상으로 분석하였다. 국민건강영양조사에서 실시되는 시력검사는 진용한시력표를 이용하고 있다. 시력의 측정은 4미터 거리에서 실시하였으며 1차 시력검사에서 나안시력이 0.8 미만인 경우 자동굴절검사(KR-8800, Topcon, Tokyo, Japan)를 사용한 굴절검사를 실시하고 이를 바탕으로 최대교정시력을 측정하여 기록한다. 약시의 기준은 단안약시의 경우 두 눈의 시력차가 2줄 이상으로 정의하였고 양안약시의 경우 기준을 0.8 미만과 0.63 미만으로 나누어 분석하였다.
자동굴절검사를 바탕으로 양안의 굴절부등약시의 경우 원시 1.5디옵터 이상, 난시 1.0디옵터 이상, 근시 3디옵터 이상으로 정의하였고 굴절약시의 경우 난시가 2.5디옵터 이상 또는 원시가 4.0디옵터 이상인 경우 의미 있는 굴절이상으로 정의하였다. 설문조사에서 시행한 환자의 거주지역과 부모의 소득 수준을 약시의 유병률과 비교 분석하였다. 소득 수준은 국민건강영양조사에서 사용한 오분위수에 의거하여 하/중하/중/중상/상으로 구분하였다.
결 과
연령별로 5세 100명(남:여=54:46), 6세 107명(남:여=59:48), 7세 106명(남:여=53:53), 8세 108명(남:여=53:55)이 포함되었다. 전체 420명(남:여=219:201) 중 약시의 유병률은 0.8 미만을 기준으로 하면 21명(5.0%), 0.63을 기준으로 설정한 경우는 16명(3.8%)이었다. 각각의 연령별 유병률은 0.8 미만을 기준으로 하였을 때는 5세에서는 10명(10.0%), 6세 6명(5.6%), 7세 4명(3.8%), 8세 1명(0.9%)로 나이가 들수록 유병률이 줄어들었으며, 0.63을 기준으로 설정한 경우에는 5세 6명(6.0%), 6세 5명(4.7%), 7세 4명(3.8%), 8세 1명(0.9%)으로 나타났다(Table 1).

Prevalence of bilateral amblyopia and unilateral amblyopia
0.8 이하를 기준으로 설정한 연구에서 의미 있는 굴절이상을 보인 경우가 전체 21명 중 9명(42.9%)이었다(Fig. 1). 의미 있는 굴절이상의 경우 단안에서는 원시부등에 의한 경우가 많았고 양안의 경우 1.5디옵터 이상의 난시로 인한 양안약시가 가장 많았다(Fig. 2). 지역별 분포는 강원도와 충청남도에서 11.1%로 가장 높게 약시 유병률이 나타났으며, 대구, 광주, 울산, 전라북도, 전라남도에서는 약시가 관찰되지 않았다(Fig. 3), 부모의 소득이 약시의 발생에 영향을 미치지는 않았다(p=0.189) (Table 2).
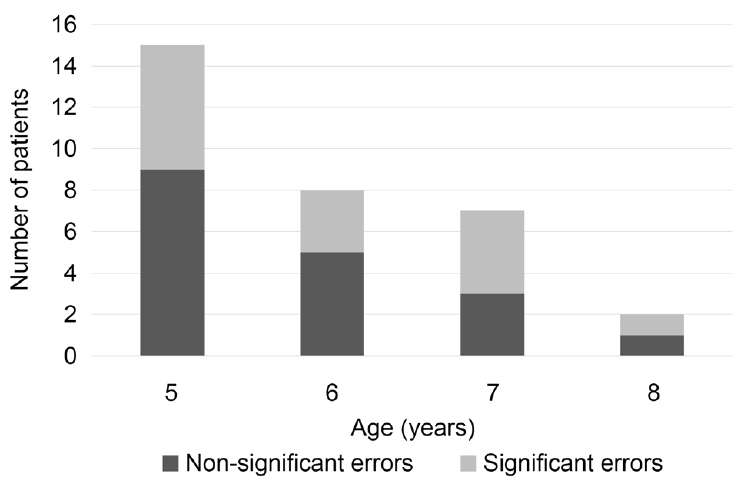
Refractive errors of the amblyopia group (less than 0.8 in the better eye and two more lines difference of visual acuity between two eyes). Significant errors are defined as follows; aniometropic amblyopia (anisohyperopia ≥ 1.5 diopters and astigmatism ≥ 1.5 diopters), bilateral amblyopia (astigmatism ≥ 2.5 diopters and hyperopia ≥ 4.0 diopters).
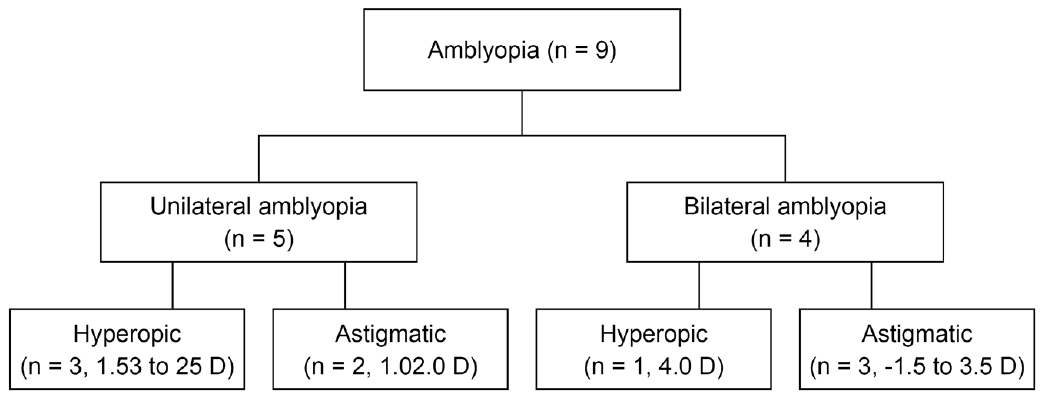
The characteristic of significant refractive errors in amblyopia. Five of nine amblyopia are unilateral amblyopia and four of nine are bilateral amblyopia. D = diopters.
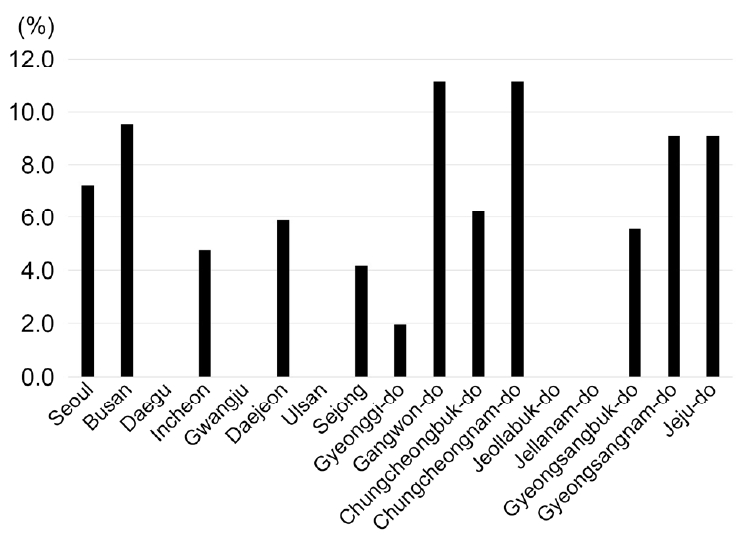
The distribution of amblyopia children. Y axis is prevalence of the amblyopia (less than 0.8 in the better eye and interocular visual acuity difference is more than 2 lines).

Status of family income between amblyopia group and normal group. No significant difference of amblyopia between two groups is found (chi-square; p = 0.189)
고 찰
2016년도에 시행한 국민건강영양조사를 통해서 알아본 5세부터 8세 소아의 약시 유병률은 5%로 나타났으며 나이가 어린 경우 유병률이 더 높게 나타난 양상을 보였다. 약시의 유병률 연구는 0.19-3.69%까지 다양하게 보고되고 있다[8-10]. 이러한 차이는 대상군의 나이, 지역, 약시의 기준에 따라 달라질 수 있음을 의미한다. 약시의 기준은 연구마다 다양하다. 일반적으로 좋은 눈의 시력이 20/30 이하를 약시로 보는 견해가 많고 약시 치료를 20/25의 시력을 목표로 하는 경우가 있어 본 연구에서는 이에 해당하는 0.63 미만과 0.8 미만 두 시력을 기준으로 나누어 분석하여 보았다[11,12]. 이번 연구에서는 0.8 미만을 기준으로는 5%, 0.63 미만을 기준으로는 3.8%로 나타났다. 다소 기존 연구보다 유병률이 높은 경향을 보이는데 이는 연구 대상의 시력 측정이 단순히 자동굴절검사에 의한 교정시력을 측정하여 다소 저교정되었을 가능성을 배제할 수 없다. 이번 연구에서는 나이가 들수록 약시의 유병률이 줄어드는 경향을 보였다. 이러한 이유는 약시가 발견되고 시간이 흐르면서 치료를 통해 약시의 유병률이 감소하였을 가능성이 있으나 이에 대한 조사는 이루어지지 않은 한계가 있다. 하지만 McKean-Cowdin et al [13]은 나이가 들수록 유병률이 다소 증가한다고 보고하였다. 이는 연령별로 약시의 기준을 48개월 미만은 20/50 미만, 48개월 이상은 20/40 미만으로 설정하여 이번 연구와는 다르게 설정된 기준 때문인 것으로 생각된다.
약시를 유발할 수 있는 위험인자는 굴절부등, 원시, 난시, 심한 근시 등과 같은 굴절이상과 사시, 그 외 백내장, 안검하수, 망막질환, 시신경 관련 질환과 같은 기질적인 질환으로 구분할 수 있으나 좁은 의미에서는 굴절이상과 사시만 약시의 원인으로 볼 수 있다[14]. 약시를 유발하는 굴절이상의 정도에 대한 연구는 다양하고 어느 정도의 굴절이상이 약시의 직접적인 원인인지 정확히 규명하기는 힘들다[3,15,16]. 따라서 약시의 기준은 연구를 진행하는 저자들의 기준에 따라 정의되고 있으나 일반적으로 굴절부등의 경우는 원시 1.5디옵터, 근시 3디옵터, 난시 1.5디옵터의 기준과 굴절약시의 경우 원시는 4디옵터, 근시 6디옵터, 난시 2.5디옵터의 기준을 많이 사용하고 이번 연구에서도 동일한 기준을 적용하였다[17,18]. 하지만 Pai et al [15]은 굴절부등의 경우 원시는 2디옵터 이상(odds ratio [OR], 15.33; 95% confidence interval [CI], 6.47-36.35), 1디옵터 이상의 난시(OR, 5.67; 95% CI, 2.53-12.71)으로 낮은 난시로 인한 굴절부등의 경우에서도 약시의 발생 가능성을 제시하였다. 이번 연구의 제한점은 조절마비굴절검사를 실시하지 않았기 때문에 원시량이 저평가되었을 가능성이 높다.
이번 약시 유병률 연구는 국민건강영양조사의 조사 방식에 따른 한계에 의해 제한점을 가지고 있다. 첫 번째로, 국민건강영양조사에서는 주기별로 다양한 검사를 선택해서 실시하고 이번 2016년도에는 시력과 굴절이상을 측정하였다. 하지만 약시를 유발할 수 있는 정밀한 사시검사, 전안부와 망막, 시신경 질환에 대한 감별진단이 빠져 있어 굴절이상이 근본적인 약시의 원인인지는 분명하지 않다. 두 번째로 일반적으로 약시를 유발할 수 있는 굴절이상의 차이를 고려하면 굴절이상에 의한 약시의 원인이 42.9%로 기존 연구들이 보고한 바와 같이 굴절이상에 의한 약시가 약 70-90%를 차지하는 결과와 차이가 있다[19-21]. 이는 국민건강영양조사에서 조절마비굴절검사를 실시하지 않아 굴절 이상이 저평가되었을 가능성이 높다. 하지만 Anker et al [16]은 선별검사의 특성상 조절마비굴절검사에 따른 시간과 보호자의 동의 문제 등을 고려하면 현성굴절검사를 이용하여 방법을 개선하면 조절마비굴절검사 없이도 선별검사로서의 가치를 갖는다고 보고하여 국민건강영양조사에서도 고려해 볼 수 있는 방법이다.
지역별 분포를 보면 표본수가 적어 통계적 분석을 내기 어려움이 있었다. Mocanu and Horhat [22]의 연구에서는 도시 지역에서 약시 유병률이 더 높다고 하였다. 이번 연구에서는 일부 지역에서 약시환아가 관찰되지 않았으나 표본 수가 적어 통계적 분석을 하기에는 어려움이 있었다. 소득층에 따른 약시 유병률의 차이는 확인되지 않았다. Sharma et al [23]은 소득이 적은 가정에서 약시평가를 위해 방문하는 기회가 적다는 점을 지적하고 관리가 필요하다고 보고하였다. 따라서 지역별, 소득 수준에 대한 정확한 평가가 이루어지려면 조금 더 소아연령대에 집중된 약시 연구가 필요할 것으로 생각된다. 또한 현재 영유아건강검진이 이루어지고 있으나 2013년도 보고 자료에 의하면 1회 이상 시각질환이 의심된 아이들이 안과검진으로 이어지는 비율이 42.4% 밖에 되지 않는다[24]. 이번 연구에서 나타난 약 3-5%로 추정되는 약시 유병률을 바탕으로 앞으로의 보건정책을 계획하고 어린 연령대에서 높게 나타난 약시 유병률을 고려할 때 만 5세 이전의 어린 연령대에서 시각검진을 실시하여 치료시기가 늦어지지 않도록 적극적인 치료를 계획하는 것이 중요하겠다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
References
Biography
윤이상 / Yisang Yoon
김안과병원
Kim’s Eye Hospital