

소실성다발백반증후군(Multiple Evanescent White Dot Syndrome, MEWDS)은 1984년 Jampol et al [1]에 의해 처음 발표된 망막색소상피층 및 맥락막의 염증성 질환으로 대개 젊은 성인 여성에서 급성, 단안성으로 발생한다. 갑작스러운 단안의 시력저하 및 시야흐림, 광시증을 주로 호소하며, 일반적으로 6주에 걸쳐 자연 회복된다고 알려져 있다[1,2]. 한 때는 감염 질환으로 알려졌으나 최근에는 유전적 감수성을 가지고 있는 사람에서 발생하는 자가 면역 질환으로 생각되고 있으며, 그 병태생리는 아직 명확히 밝혀져 있지 않다[3-5].
최근 여러 비전형적 증례들이 보고됨에 따라 소실성다발백반증후군의 진단에 있어서 다양한 검사법의 통합적 사용이 중요시되고 있다[6-8]. 전형적인 안저 소견으로는 다발성 백색반점이 주로 후극부에 발생하며 중심와 부위의 입자형병변(foveal granularity)이 관찰되며, 자가형광촬영에서는 급성기에 백색반점 부위가 저형광을 보이다가 회복기에 들면서 소실되거나 과형광으로 바뀌게 된다. 형광안저혈관조영술(fluorescein angiography)상 초기와 후기 모두 과형광 소견을 보이고, 인도사이아닌그린혈관조영술(indocyanine green angiography)에서는 초기에는 특이 소견이 없거나 과형광을 보이다가 후기에는 저형광을 보이는 것이 특징적이다. 최근 빛간섭단층촬영(optical coherence tomography)이 상용화되면서 백색반점 부위의 망막상피세포층은 비교적 정상 소견을 보이나 바깥 망막층에는 타원체구역(ellipsoid zone)에 집중된 다발성 침착물을 보이는 것을 특징으로 한다. 본 증례의 환자는 이러한 기존의 알려진 자연경과와는 다르게, 급성기 반점이 없던 부위에 회복기 색소침착이 발생하고 시간이 경과함에 따라 색소침착이 소실되는 것을 경험하였기에 보고하고자 한다.
증례보고
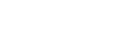
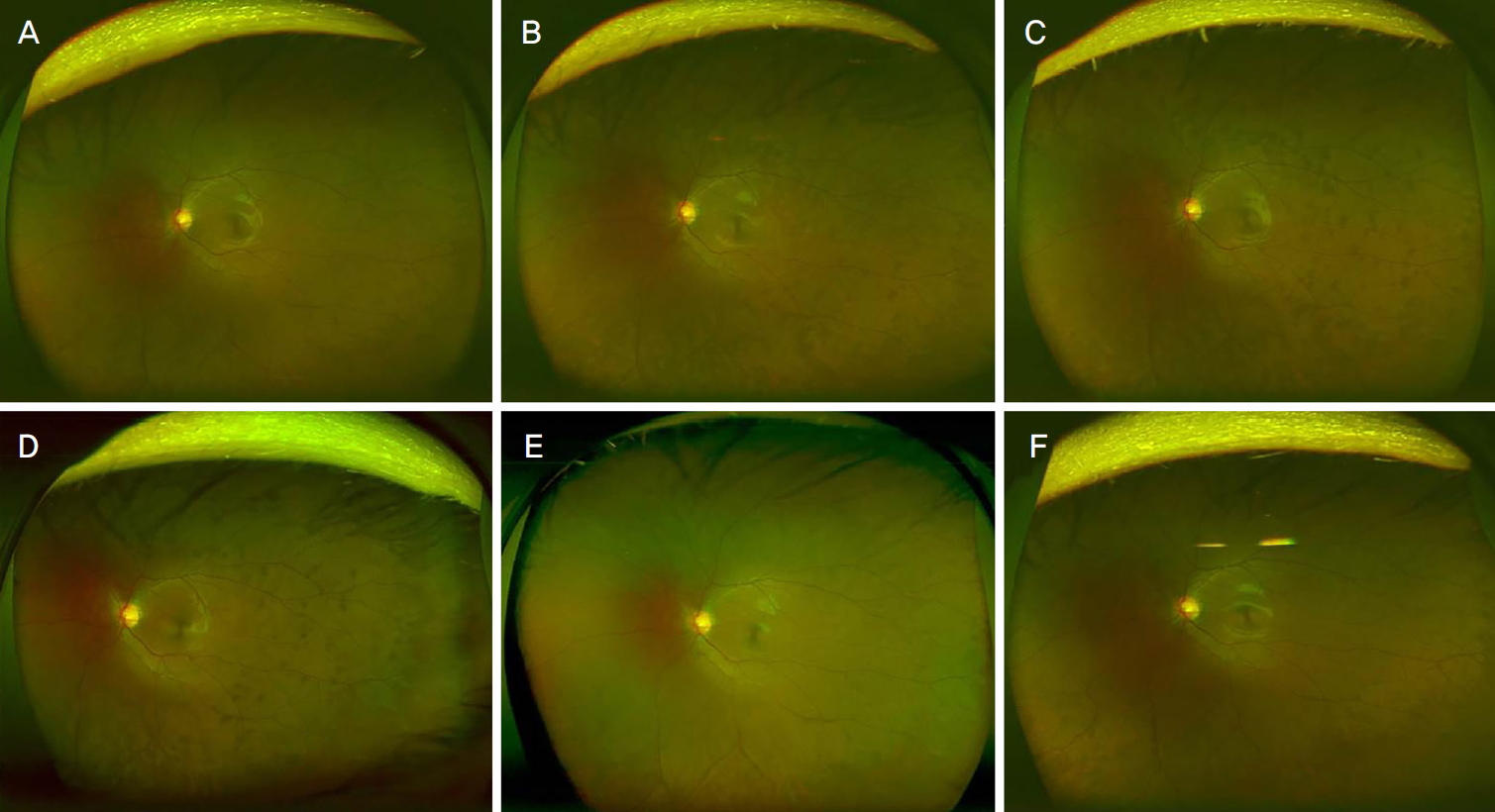
특이 전신질환이 없는 17세 남자가 좌안의 시력저하를 주소로 내원하였다. 시력검사상 최대교정시력 우안 1.0, 좌안 0.5였고 안압은 우안 14 mmHg, 좌안 12 mmHg였다. 안저검사상 우안은 정상 소견을 보였으나, 좌안의 비측 망막에 다수, 황반 주위로 소수의 경계가 불분명한 백색반점이 관찰되었고, 자가형광촬영에서 백색반점 부위 및 시신경 주위로 과형광 소견을 보였다(Fig. 1A, B). 형광안저혈관조영술에서 초기에 주로 시신경 유두의 비측과 상측에서 과형광 점들이 관찰되었으나 중기로 갈수록 초기에는 뚜렷하게 병변이 보이지 않았던 황반 주위로 과형광 병변들이 나타났으며, 후기에 들면서 점점 더 뚜렷해지면서 전형적인 고리형 화환 모양(wreath like hyperfluorescence)을 보였다. 인도사이아닌그린혈관조영술에서 초기에는 특이 소견이 없었으나 후기에는 형광안저혈관조영술의 과형광 병변들에 상응하는 부위에 저형광 병변이 명확히 관찰되었다(Fig. 1C-E). 또한, 빛간섭단층촬영상 중심와 부위의 타원체구역이 불규칙해지고 국소적인 소실을 보였다(Fig. 1F). 상기 소견들을 종합하였을 때, 소실성다발백반증후군으로 생각되어 특이 약물치료 없이 경과 관찰하기로 하였다.
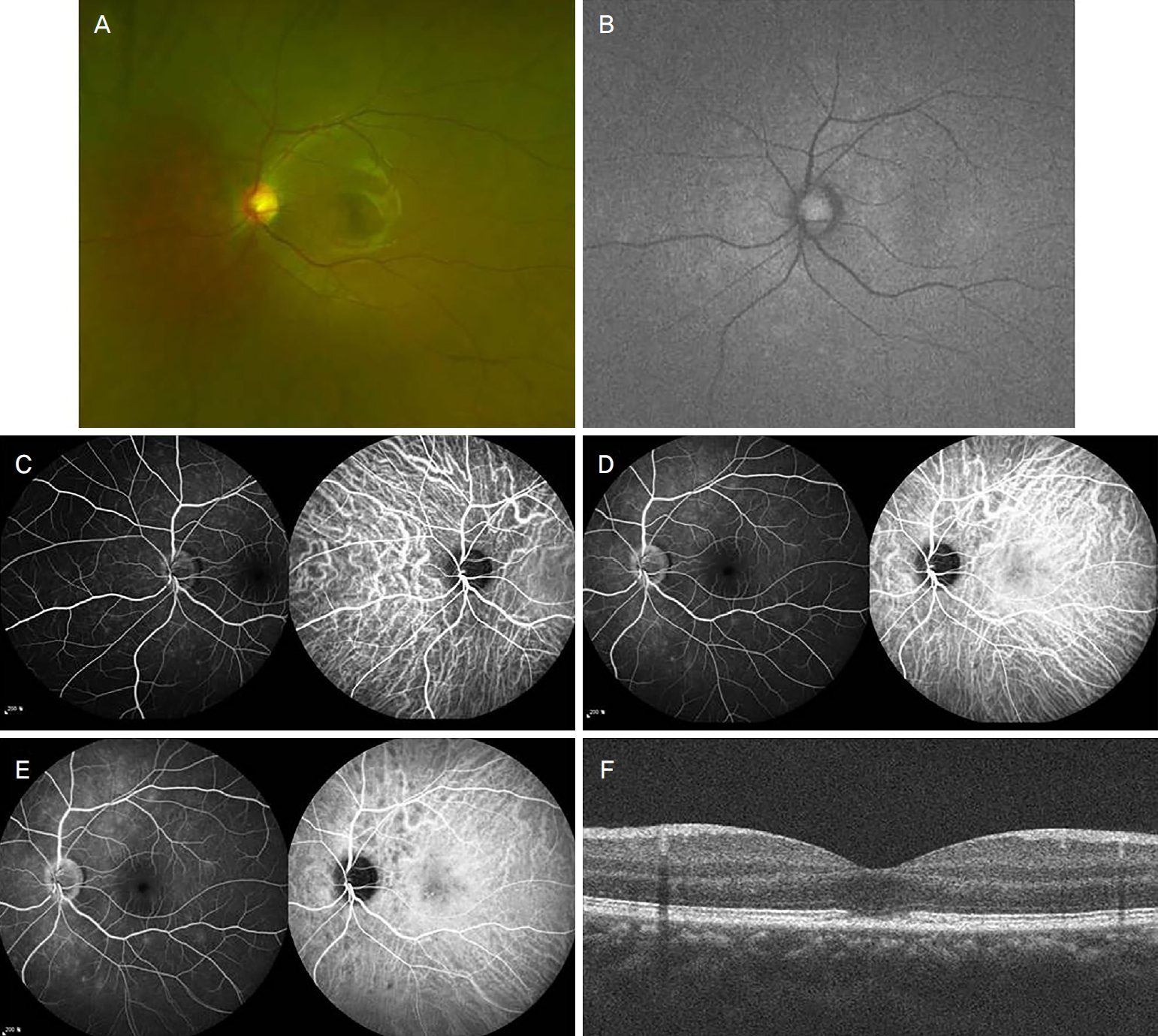
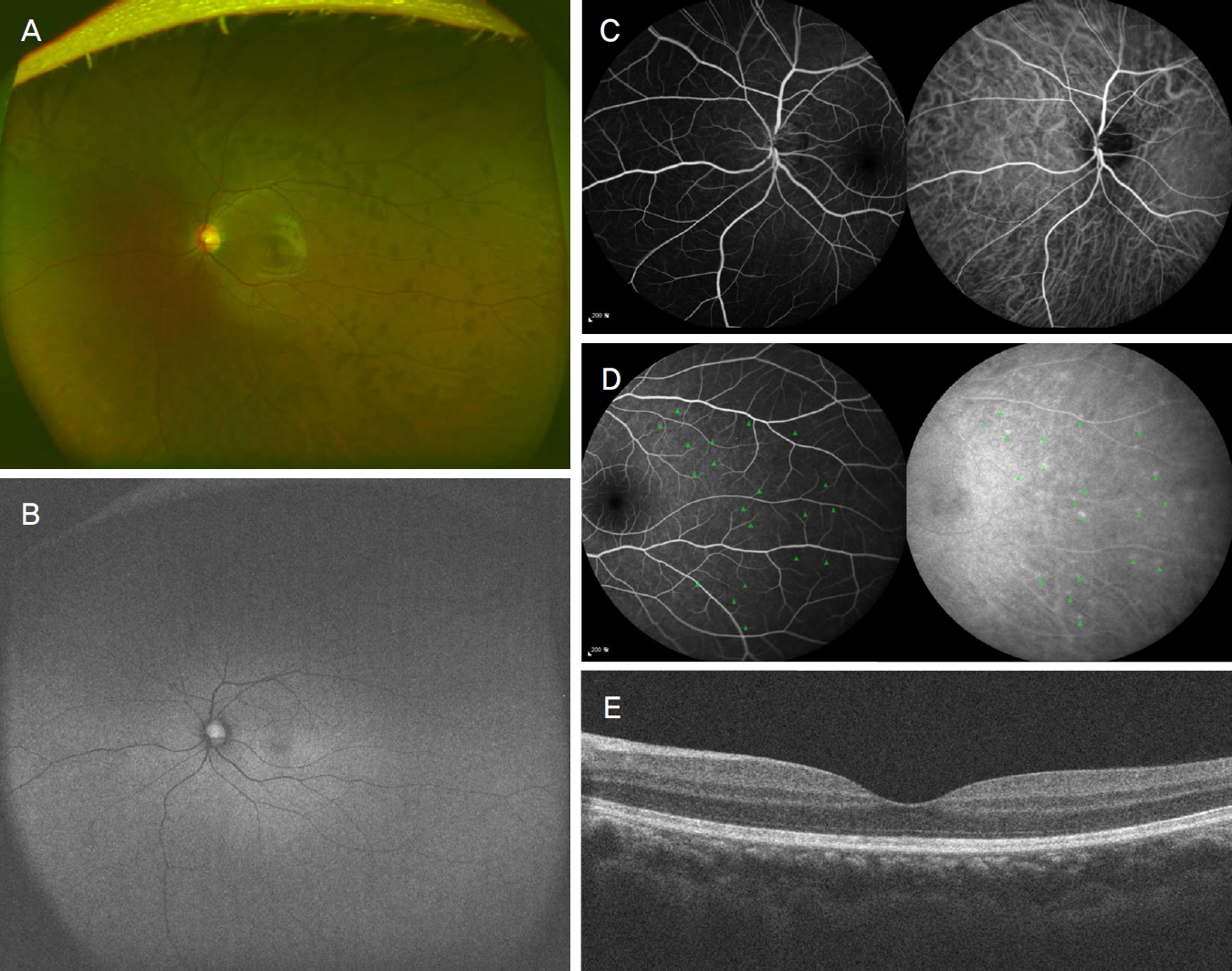
내원 6주 후 좌안 최대교정시력 1.0으로 완전하게 호전되었으며, 안저검사상 기존의 백색반점은 거의 소실되었다. 그러나 색소침착반점이 망막 전 영역에 걸쳐 모세혈관을 따라 산발적으로 그 말단에 분포하는 양상을 보였다(Fig. 2A). 자가형광촬영상 기존의 과형광 병변은 소실되었다(Fig. 2B). 형광안저혈관조영술 및 인도사이아닌그린혈관조영술 초기에 기존의 과형광 병변들이 모두 소실되었으나, 조영 후기에 이측으로 안저촬영상 색소침착 병변의 위치와 상응하는 곳에 형광안저혈관조영술에서는 저형광 병변이, 인도사이아닌그린혈관조영술에서는 다수의 과형광 병변이 관찰되었다(Fig. 2C, D). 빛간섭단층촬영상 소실되었던 중심와 부위의 타원체구역 형태는 정상화된 반면(Fig. 2E), 색소침착이 있는 부위는 타원체구역의 신호가 감쇄(attenuation)된 소견을 보였다(Fig. 3). 내원 9주 후 경과 관찰 시 안저검사상 색소침착은 점차 감소하는 양상을 보였고 이후 2개월동안 색소침착 병변도 지속적으로 감소하여 소실되었으며, 어떠한 반흔 조직도 남기지 않았다(Fig. 4).
고 찰
소실성다발백반증후군의 일반적인 안저 소견은 특히 황반 주위와 망막 중간주변부 영역에서 발견되는 다수의 100-200 µm 크기의 경계가 불분명한 흰색 또는 노란색 반점을 보인다. 빛간섭단층촬영 및 형광안저혈관조영, 인도사이아닌그린혈관조영검사 결과 이 반점들은 바깥 망막층(outer retinal layer)에 분포하는 것으로 관찰되며 수주 후 자연 소실되는 것을 특징으로 한다[1-3].
위와 같이 전형적인 임상양상을 보이지 않고, 비전형적인 다발성소실성백반증후군 임상양상을 보이는 증례가 일부 보고되고 있다. Shelsta et al [9]은 급성기 백색반점이 뚜렷하게 나타나지 않은 증례 3예를 보고하였고, Huang and Spaide [10]는 본 증례와 비슷하게 백색반점과 색소침착이 서로 다른 부위에서 관찰되었으나, 이후에 망막 주변부로 새로운 병변 발생과 함께 초기의 백색반점이 점차 색소침착으로 변하는 경과를 보이는 증례를 보고하였다. 두 증례와는 다르게 본 증례의 환자는 백색반점과 색소침착이 서로 다른 부위에, 그리고 급성기와 회복기라는 서로 다른 시기에 발생했다는 점이 기존의 비전형적인 자연경과를 보이는 보고들과는 차이가 있다.
본 증례에서 단안의 시력저하와 함께 안저촬영, 자가형광촬영, 형광안저혈관조영술 및 인도사이아닌그린혈관조영술에서 기존에 알려진 특징적 급성기 소견들이 모두 관찰되고 최종적으로 시력이 완전히 회복되는 등 소실성다발백반증후군의 자연 경과를 보인다. 그러나 급성기의 백색반점은 흔적 없이 소실되고 회복기에 전혀 다른 위치에 색소침착 반점이 발현된 비전형적 임상양상을 보이는 증례라 할 수 있다. 이러한 질병 경과가 발생하게 된 기전에 대해서 명확하게 밝히기는 아직 어렵다. 본 증례에서 색소침착이 급성기 백색반점과는 떨어진 모세혈관을 따라 망막 전 영역에 분포하는 점을 주목하였을 때, 색소침착은 자가 면역 반응에 의한 염증매개로 인한 것으로 추측된다. 이러한 가설은 추후 연구를 통해 그 기전이 밝혀져야 하겠다.
소실성다발백반증후군에서 급성기 백색반점과 다른 부위에 회복기 색소침착이 발생할 수 있고, 이러한 색소침착이 시간이 경과함에 따라 반흔으로 변화 없이 소실될 수 있음을 보여주는 최초의 보고이다. 이러한 비전형적인 양상이 소실성다발백반증후군의 자연 경과에 영향을 주지 않으므로 그 진단과 치료에 있어 비전형적 양상 발생 가능성에 염두에 두어야 하겠다.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






