

원발급성폐쇄각발작(acute primary angle closure)은 갑작스러운 홍채에 의한 섬유주의 해부학적 폐쇄로 방수의 흐름이 차단되면서 안압이 상승하는 질환으로, 동아시아에서 흔하다[1-5]. 이환된 눈의 시야흐림, 통증, 충혈이 발생할 수 있고, 심할 경우 오심, 구토 증상이 동반되며, 안과적 응급 질환으로 분류되기도 한다[2,5]. 일반적으로 원발급성폐쇄각 발작의 치료는 안압을 하강시키는 약물치료와 함께 레이저 홍채절개술(laser iridotomy)을 시행하는데, 신속한 치료로 급성 증상 및 징후가 해소된 경우라도 이후 비가역적인 시신경, 망막 손상이 유발될 수 있다[6-9]. 이런 비가역적인 시신경 손상을 시신경의 관류와 망막신경절세포 축삭의 손상과의 상호작용으로 설명하기도 하지만 정확한 기전과 영향을 미치는 요소에 관해서는 아직 확실히 밝혀지지 않았다[10-12].
빛간섭단층혈관조영술(optical coherence tomography angiography, OCTA)은 시신경과 망막모세혈관 구조에 대한 빠르고 비침습적인 고해상도의 검사를 가능하게 한다. 내장된 소프트웨어를 이용하여 측정 영역의 단위면적당 혈관의 총 길이를 의미하는 혈관밀도(vessel density)와 단위면적당 혈관의 총 넓이를 뜻하는 관류밀도(perfusion density)를 측정하고, 이를 통해 시신경과 망막의 모세혈관분포와 관류에 대해 분석할 수 있다. 이는 일반적인 형광혈관조영술과 잘 일치하며 상세한 해부학적 및 관류에 대한 정보를 제공한다고 알려져 있다[13,14].
원발개방각녹내장(primary open angle glaucoma)에서 망막신경섬유층(retinal nerve fiber layer), 신경절-내망상층(ganglion cell-inner plexiform layer)의 두께 감소와 같은 구조적인 변화와 함께 빛간섭단층혈관조영술을 통해 시신경과 황반부 주위의 모세혈관분포의 변화가 확인되었고, 시신경유두주위 혈액 관류의 장애가 녹내장성 시신경 손상을 일으킬 수 있다는 가능성이 보고되었다[15-19]. 또한 Moghimi et al [12]는 단안의 급성폐쇄각발작 해소 후 8주째 병변안의 시신경유두주위 망막신경섬유층 두께가 대조군인 반대안에 비해 감소함과 함께 시신경유두주위 혈관밀도 또한 유의하게 감소함을 확인하였다. Wang et al [20]은 원발급성폐쇄각발작안과 원발폐쇄각녹내장의증(primary angle closure suspect)인 반대안에서 급성 발작 이후 망막신경섬유층, 신경절-내망상층 두께는 두 군에서 유의한 차이가 없었으나, 시신경유두주위 혈관밀도의 경우 병변안에서 유의하게 낮았음을 보고하였다.
그러나 원발급성폐쇄각발작안에서 망막모세혈관분포의 변화와 관련된 연구는 아직 제한적이며, 명확한 관련성은 확인되지 않았다. 급격한 안압상승이 망막에 허혈성 손상을 야기할 수 있으므로 본 연구에서는 원발급성폐쇄각발작 후 시신경유두주위와 황반부의 모세혈관분포를 알아보고자 하였다[21,22]. 급성폐쇄각발작 해소 이후에 시신경유두주위, 황반부의 녹내장성 구조적인 변화를 보이지 않았던 경우를 대상으로 안압상승의 과거력이 없었고, 시신경과 망막의 녹내장성 변화가 관찰되지 않았던 반대안을 대조군으로 하여 시신경유두주위와 황반부의 모세혈관분포의 차이를 분석하였다.
대상과 방법
본 연구는 헬싱키선언에 입각한 의학연구윤리심의위원회의 승인을 받고(승인 번호: 20-0071) 연구관련 심의 규정 및 지침에 따라 진행되었다. 2018년 1월부터 2019년 12월까지 단일 기관에 내원하여 단안 원발급성폐쇄각발작을 진단받고 안압하강제 점안 및 레이저홍채절개술을 통해 증상과 징후가 호전되었던 20명의 환자를 대상으로 발병안과 원발급성폐쇄각발작이 발생하지 않은 반대안을 대조군으로 하여 후향적으로 의무기록을 분석하였다. 원발급성폐쇄각발작은 초진 당시 골드만압평안압계로 측정한 안압이 30 mmHg 이상이며, 전형적인 증상(안구통증, 두통, 시력, 오심, 구토 등)을 호소하는 환자 중 세극등현미경검사에서 각막부종, 결막충혈, 얕은 전방(중심 전방깊이가 각막두께의 3배 이하, 이측 주변부 전방깊이가 각막두께의 1/4배 이하)과 중등도로 산동된 동공이 관찰되고, 전방각경검사에서 전방각이 270° 이상 좁아진 경우에서 진단하였다[23].
연구 대상자의 선정 기준은 1) 양안 전방이 얕은 경우, 2) 단안에만 원발급성폐쇄각발작이 발생한 경우, 3) 안압하강제 점안 및 레이저홍채절개술을 시행한 직후 성공적으로 안압하강(21 mmHg 이하) 및 증상 호전이 이루어진 경우, 4) 안압하강 후 8주경 시행한 빛간섭단층촬영에서 시신경과 황반부의 녹내장성 구조적인 변화가 관찰되지 않는 경우로 정하였고, 4가지를 모두 만족하는 환자를 연구 대상에 포함시켰다. 이전에 양안에 녹내장을 진단받은 적이 있거나 시행한 검사(안저검사, 빛간섭단층촬영, 시야검사)에서 녹내장성 병변이 저명한 경우, 급성폐쇄각발작 과거력이 있는 경우, 포도막염, 술 후 합병증 등 다른 원인에 의해 발생한 급성폐쇄각발작인 경우, 안구내 수술 기왕력이 있는 경우는 연구 대상에서 제외하였다.
연구 대상자들은 모두 초진 시 병력 조사, 골드만안압검사, 세극등현미경검사, 전방각경검사를 시행하였고, 급성폐쇄각발작 후 안압하강제 점안 및 레이저홍채절개술을 시행하였다. 이후 모든 환자들은 급성폐쇄각발작 치료 후 6-12주 내에 재내원하였고, 골드만안압검사, 세극등현미경검사와 더불어 양안 최대교정시력, 굴절검사를 시행하였다. 추가적으로 양안 산동 후 안저검사, 스펙트럼 영역 빛간섭단층촬영검사(spectral domain optical coherence tomography) 및 빛간섭단층혈관조영술을 시행하였다. 빛간섭단층촬영기(Cirrus™ HD-OCT; Carl Zeiss Meditec, Dublin, CA, USA)의 내장된 소프트웨어 중 optic disc cube 200 × 200 스캔과 macular cube 512 × 128 스캔, ganglion cell analysis (GCA) 알고리즘을 이용하여 시신경유두주위 망막신경섬유층과 황반부 신경절-내망상층의 두께를 분석하였다. Optic disc cube scan을 이용하여 유두 중심을 기준으로 하는 3.46 mm의 직경을 가지는 원에서 평균 망막신경섬유층 두께 및 구역별(상측, 상이측, 하이측, 하측, 하비측, 상비측) 두께를 분석하였고, macular cube 스캔과 GCA 알고리즘을 이용하여 황반부를 중심으로 하는 14.13 mm2의 타원형 도넛 모양 영역의 평균 신경절-내망상층 두께와 구역별(상측, 상이측, 하이측, 하측, 하비측, 상비측) 두께를 측정하여 양안을 비교하였다[14,24-26]. 측정의 정확성을 위해 신호 강도가 6점 이상인 결과만을 분석 대상에 포함시켰다.
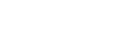
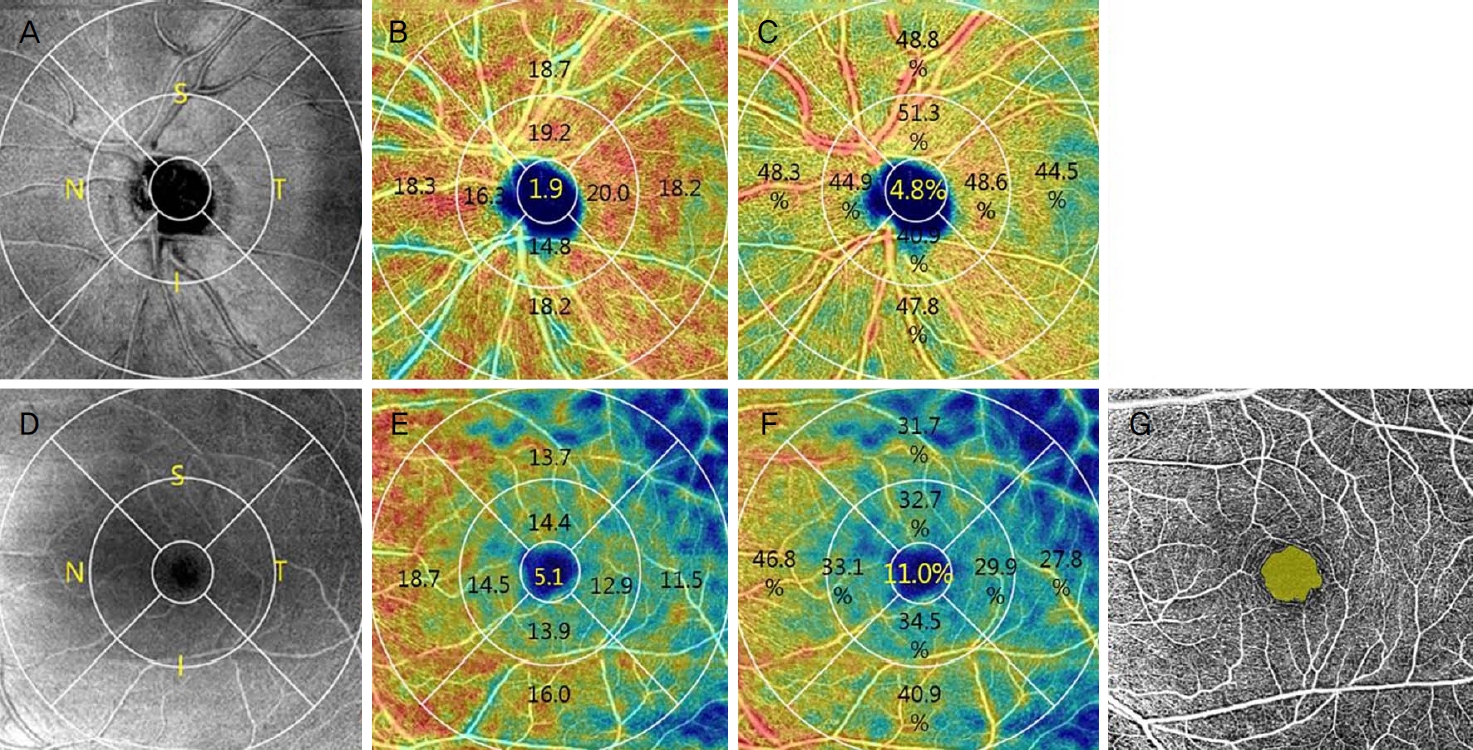
빛간섭단층혈관조영술의 경우 Cirrus OCTA 소프트웨어(AngioPlex version 10.0; Carl Zeiss Meditec, Dublin, CA, USA)를 사용하여 연속적인 B-scan을 시행하며 적혈구의 움직임을 감지함으로써 시신경유두 및 황반부의 혈관분포를 분석하였다[27]. Early treatment diabetic retinopathy study (ETDRS) 영역을 적용하여 6 × 6 mm 스캔 영역을 시신경유두(optic nerve head)와 황반오목의 중심으로부터 1) 반경 0.5 mm 이내의 중심 영역(center), 2) 반경 0.5-1.5 mm 범위의 고리 모양 안쪽 영역(inner), 3) 반경 1.5-3.0 mm 범위의 고리 모양 바깥쪽 영역(outer), 4) 반경 3 mm 이내의 전체 영역(total)으로 나누고, 안쪽과 바깥쪽 영역을 상측, 이측, 비측, 하측으로 한 번 더 나누어 각각의 혈관밀도와 관류밀도를 측정하였으며, 황반부 오목무혈관부위(foveal avascular zone)의 면적과 둘레를 확인하였다(Fig. 1) [28,29]. 통계 분석은 SPSS version 24.0 (IBM Corp., Armonk, NY, USA)을 이용하였고, Wilcoxon signed rank test를 사용해 양군의 연속형 자료를 비교 분석하였으며, p-value가 0.05 미만인 경우를 통계학적으로 유의한 것으로 판정하였다.
결 과
대상 환자들의 평균 나이는 62.50 ± 5.85세(51-74세)였고, 남자가 5명, 여자가 15명이었다. 초진 시 골드만압평안압계로 측정한 평균 안압은 병변안에서 45.75 ± 12.12 mmHg, 반대안에서 14.95 ± 2.87 mmHg로 병변안에서 유의한 안압 상승을 보였다(p<0.001). 급성폐쇄각발작 후 치료를 시행하기까지 걸린 기간은 평균 31.70 ± 23.45시간이었고, 급성폐쇄각발작 해소 후 빛간섭단층촬영과 빛간섭단층혈관조영술을 시행하기까지 걸린 기간은 평균 8.30 ± 2.36주였다. 초진시 원발급성폐쇄각발작안의 안압과 급성폐쇄각발작 해소 후 평균 8주째 원발급성폐쇄각발작안의 안압을 비교하였을 때 안압의 유의한 감소를 보였다(p<0.001). 급성폐쇄각발작 후 8주째 양안의 안압을 비교하였을 때는 병변안에서 14.70 ± 3.51, 반대안에서 13.35 ± 2.62 mmHg로 유의한 차이가 없었다. 최대교정시력과 굴절률 또한 양안에서 차이를 보이지 않았다(Table 1).
고 찰
원발급성폐쇄각발작에서 발생하는 녹내장성 시신경 손상은 높은 안압으로 인한 시신경의 물리적인 압박이 주된 기전으로 받아들여지고 있다[30,31]. 하지만 혈관인자 역시 녹내장성 시신경 손상을 일으킬 수 있다는 가정 아래 여러 연구들이 진행되었다[12,32-35]. 본 연구에서 원발급성폐쇄각발작안과 반대안을 비교하였을 때 시신경유두주위 망막신경섬유층, 황반부 신경절-내망상층의 두께는 차이가 없었으나, 황반오목으로부터 0.5 mm 내의 중심영역에서 혈관밀도와 관류밀도가 유의하게 감소하였다. 이는 갑작스러운 안압상승이 시신경과 황반 모두에게 기계적인 압박을 하였으나 녹내장성 구조적 손상을 일으키지는 못하였고, 허혈에 취약한 황반 중심부의 혈관인자에 영향을 준 것으로 생각된다. 그러나 황반부 오목무혈관부위의 면적과 둘레의 경우는 양안에서 유의한 차이가 없었다. 황반부 오목무혈관부위는 모세혈관이 분포해 있지 않은 원형의 부위로 크기와 모양은 황반부 모세혈관의 변성이나 위축에 영향을 받으며 당뇨망막병증이나 망막정맥폐쇄 같은 망막질환의 진단적 가치를 지니고 허혈 범위를 예측할 수 있다[36-38]. 갑작스러운 안압상승이 황반부 오목무혈관부위의 경계에 위치한 모세혈관의 구조적 손상을 일으키지 않았다면 황반부 오목무혈관부위의 둘레와 넓이에는 차이가 없을 수 있다고 생각한다. 하지만 본 연구에서는 대상안의 수가 적었기 때문에 향후 갑작스러운 안압상승이 황반부 오목무혈관부위와의 둘레와 넓이에 미치는 영향에 관한 연구가 추가적으로 필요할 것이다.
단안 원발폐쇄각녹내장 환자군을 대상으로 한 연구에서 병변안의 시신경유두주위 혈관밀도가 유의하게 감소하였고, 이는 망막신경섬유층과 신경절-내망상층 두께와 유의한 관련성을 가진다고 보고하였다[32]. 또한 Zhu et el [33]은 원발폐쇄각녹내장 환자군에서 시신경유두주위와 황반부의 모든 영역에서 유의한 혈관밀도의 감소를 보였고, 시신경유두주위 영역에서의 혈관밀도의 감소량이 황반부의 혈관 밀도의 감소량보다 많다고 보고하였다. 본 연구에서는 원발급성폐쇄각발작 후에도 구조적으로 녹내장성 변화가 보이지 않았던 눈을 대상으로 하였으므로 구조적인 변화가 있었던 원발폐쇄각녹내장 환자를 대상으로 한 연구 결과들과는 차이가 있을 것으로 생각한다.
Moghimi et al [12]의 연구에서는 원발급성폐쇄각발작 후 8주째 시신경유두주위 망막신경섬유층 두께와 시신경유두주위 혈관밀도 모두 감소함을 확인하였고, 시신경유두주위 혈관밀도의 변화가 시신경유두주위 망막신경섬유층의 두께 감소 진행과 유의한 상관관계를 보이는 유일한 변수임을 보고하였다. 원발급성폐쇄각발작안과 반대안, 정상안을 비교한 연구에서는 급성폐쇄각발작 후 1주와 6주째 시신경유두주위 혈관밀도를 분석하였고, 모두 병변안에서 유의하게 낮은 결과를 보였다[34]. 시신경유두주위 망막신경섬유층 두께의 경우 1주째에는 병변안에서 오히려 증가하였으며, 6주째 다시 감소하는 결과를 보였다. 이를 통해 시신경유두주위 혈관밀도가 망막신경섬유층의 구조적 변화보다 선행할 수 있음을 보고하였다. 두 연구 모두 원발급성폐쇄각발작을 대상으로 한 연구였으나, 병변안의 구조적인 변화가 있는 상태에서의 혈관밀도에 관한 분석이기 때문에 본 연구의 결과와 차이가 있을 수 있다.
Wang et al [20]은 급성폐쇄각발작 해소 후 망막신경섬유층, 신경절-내망상층 두께는 병변안과 반대안에서 유의한 차이가 없었고, 시신경유두주위 혈관밀도의 경우 원발급성폐쇄각발작안에서 유의하게 낮았음을 확인하였다. 또한 시야검사를 시행하여 원발급성폐쇄각발작안에서 유의한 mean deviation의 감소와 pattern standard deviation의 증가를 확인하였고, 이는 시신경유두주위 혈관밀도와 유의한 상관관계가 있음을 밝혔다. 구조적인 변화에 선행하여 시신경의 모세혈관분포의 변화가 있었다는 점에서 본 연구 결과와 공통된 부분이 있지만, 시신경유두주위 혈관 인자와 관련된 분석 결과는 본 연구 결과와 상이하였다. Wang et al [20]의 연구에서는 급성폐쇄각발작 해소 후 평균 16.5일에 빛간섭단층혈관조영술을 시행하였고, 검사 시점에서 안압상승으로 인한 망막부종으로 시신경유두주위 망막신경섬유층과 황반부 신경절-내망상층 두께가 증가되어 녹내장성 구조적인 변화가 가려졌을 가능성을 고려하여야 하겠다[12,34].
Rao et al [35]는 원발폐쇄각녹내장 환자의 경우 정상안인 대조군과 비교하였을 때 망막신경섬유층, 신경절-내망상층의 두께와 시신경유두주위, 황반부 혈관밀도가 모두 유의하게 감소하였음을 확인하였다. 그러나 안압이 21 mmHg를 초과한 적이 있지만 녹내장으로 진행되지 않은 원발폐쇄각(primary angle closure) 환자에서는 상이측 망막신경섬유층 두께의 유의한 감소만 있었고, 혈관밀도는 시신경유두주위와 황반부의 모든 영역에서 대조군과 차이가 없었다. 이 연구는 급성폐쇄각발작의 과거력이 없는 원발폐쇄각녹내장안과 원발폐쇄각안을 대상으로 진행되었기 때문에 본 연구 결과와 차이가 있을 것으로 생각된다.
시신경의 상이측, 하이측 망막신경섬유층에서 녹내장성 구조적인 손상이 흔히 발생하며, 황반부 신경절-내망상층의 이측 부위 또한 녹내장성 변화에 취약하다고 알려져 있다[39,40]. 그러나 높은 안압상승을 보이는 폐쇄각녹내장의 경우 녹내장성 손상의 양상이 다르다는 보고가 있다[21,34,41]. 급성폐쇄각발작에서 발생하는 높은 안압상승은 수정체, 각막내피세포, 홍채 등 여러 안내 구조에 허혈성 손상을 유발하고 시신경 주변, 황반 주변 미세혈관 관류에 영향을 줄 수 있다[22]. 본 연구에서는 황반부 중심 영역 내의 혈관밀도와 관류밀도가 감소하였는데 이는 황반부는 오직 망막동맥에 의해서만 혈액 공급을 받고, 다른 조직에 비해 산소 소비량이 높아 허혈성 손상에 취약하기 때문일 것으로 생각된다[42,43].
원발급성폐쇄각발작안에서 혈관 인자를 분석한 연구는 많지 않고, 구조적인 변화가 일어나지 않은 급성폐쇄각발작안에서 혈관 인자를 분석한 연구는 더욱 제한적이다. 급성폐쇄각발작 해소 후에 구조적인 변화가 나타나지 않았음에도 황반부 혈관밀도와 관류밀도의 감소가 있었던 본 연구 결과는 안압의 일시적인 상승이 구조적인 변화보다 먼저 모세혈관분포의 변화를 일으킬 수 있는 가능성을 시사한다. 따라서 급성폐쇄각발작안에서 증상이 호전된 후 녹내장성 구조적 손상이 발견되지 않았더라도 황반부 모세혈관분포가 감소할 수 있으므로 구조적인 변화로 이어지는지에 대한 지속적인 경과 관찰이 필요하다고 생각된다.
여러 연구에서 황반부의 ETDRS 영역에 따른 망막의 구조적인 차이가 있음이 밝혀졌으며, 본 연구에서는 이를 토대로 구역별 모세혈관분포의 차이를 가정하여, 황반부를 오목무혈관부위와 중심와를 고려한 직경이 다른 세 개의 동심원으로 구분지었다[44]. 시신경유두주위 영역에서도 시신경유두로부터 분지하는 망막혈관의 분포를 고려하여 시신경유두와 유두주위를 같은 방식으로 구분지었고, 이를 통해 병변안의 황반부 중심영역에서 유의하게 낮은 혈관밀도와 관류밀도를 확인할 수 있었다. 녹내장 환자의 시신경유두주위 또는 황반부의 혈관 인자를 영역에 따라 분석한 연구는 제한적이었으며, 국소적인 변화를 알 수 있었다는 점에서 본 연구는 의미가 있다고 생각한다. 또한 장기적인 관찰이 이루어진다면 병의 진행에 따른 영역별 혈관인자의 변화를 확인할 수 있을 것이라 기대한다.
본 연구는 3차 상급종합의료기관에 내원하여 치료 받은 환자의 의무기록을 후향적으로 분석하였고 대상 환자의 수가 상대적으로 적어 선택 비뚤림 가능성이 있을 수 있다. 이전 병력에 대한 확인이 문진에 의해 이루어졌기 때문에, 원발급성폐쇄각발작 과거력의 가능성을 완전히 배제하진 못하지만 녹내장성 구조적 변화가 없었던 경우를 대상으로 하였으므로 이전의 원발급성폐쇄각발작 가능성은 낮을 것으로 생각된다. 급격한 안압상승에 대한 망막모세혈관분포의 변화를 보기 위해서는 발병 전과 후를 비교해야 하지만, 안압상승 시기를 예측할 수 없었기 때문에 급성폐쇄각발작 이후 병변안과 안압상승의 과거력이 없는 반대안을 비교 분석하였다[45]. 따라서 모세혈관분포의 차이와 급성폐쇄각발작 사이의 선후관계는 확인할 수 없었다. 가능하다면 급성폐쇄각발작 전과 후의 변화에 대한 추가 연구가 필요할 것으로 생각된다.
결론적으로 원발급성폐쇄각발작 후 망막신경섬유층, 신경절-내망상층의 두께 감소 등의 구조적인 변화가 관찰되지 않았던 눈에서 황반부 혈관밀도와 관류밀도의 감소를 확인하였다. 이는 단기간의 높은 안압이 녹내장성 구조적 손상을 일으키지는 않더라도 황반부의 모세혈관분포에 영향을 줄 수 있음을 의미한다. 따라서 망막모세혈관밀도 및 관류밀도의 감소가 구조적 손상에 선행할 가능성을 고려하여 급성폐쇄각발작 후 녹내장성 구조적 손상이 보이지 않는 경우라도 구조적인 변화가 발생하는지에 대한 주의 깊은 관찰이 필요할 것이다.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






