

1971ļģä Urayama [1]ņŚÉ ņØśĒĢ┤ ņ▓śņØī ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ļØ╝ļŖö ņ¦łĒÖśņØ┤ ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░, Ēśäņ×¼ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ļŖö ņĢłĻĄ¼ļé┤ ņŚ╝ņ”Øņ¦łĒÖśņ£╝ļĪ£, ĒĢŁļ░öņØ┤ļ¤¼ņŖż ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņØä Ļ▓ĮņÜ░ ļ╣Āļź┤Ļ▓ī ņ¦äĒ¢ēĒĢśļŖö ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēĻ┤┤ņé¼ņÖĆ ĒÅÉņćäĒśłĻ┤Ćļ│æņ”Ø, ņĀäļ░® ļśÉļŖö ņ£Āļ”¼ņ▓┤ņØś ņŚ╝ņ”ØņØä ļÅÖļ░śĒĢśļŖö ņ¦łĒÖśņØ┤ļŗż. ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņØś ņøÉņØĖņ£╝ļĪ£ļŖö ņłśļæÉļīĆņāüĒżņ¦äļ░öņØ┤ļ¤¼ņŖż(varicella zoster virus)Ļ░Ć Ļ░Ćņן ļ¦ÄņØĆ ļ╣äņ£©ņØä ņ░©ņ¦ĆĒĢśļ®░, ļŗ©ņł£Ēżņ¦äļ░öņØ┤ļ¤¼ņŖż 1ĒśĢ(Herpes simplex virus type I, HSV-1)Ļ│╝ 2ĒśĢ(HSV-2)ņØ┤ ĻĘĖ ļŗżņØīņØä ņ░©ņ¦ĆĒĢ£ļŗż[2]. ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņØś ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ļŖö ĒĢŁļ░öņØ┤ļ¤¼ņŖżņĀ£ ņĀĢļ¦źņŻ╝ņé¼, ĒĢäņÜö ņŗ£ ņ£Āļ”¼ņ▓┤Ļ░Ģļé┤ ĒĢŁļ░öņØ┤ļ¤¼ņŖżņĀ£ ņŻ╝ņé¼, ņןļ▓ĮļĀłņØ┤ņĀĆņłĀ, ļ¦Øļ¦ēļ░Ģļ”¼Ļ░Ć ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░ ņłśņłĀ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ļŗż[3]. ĒĢŁļ░öņØ┤ļ¤¼ņŖż ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņØä Ļ▓ĮņÜ░ ļ│æļ│ĆņØ┤ ĻĖēņåŹļÅäļĪ£ ņ¦äĒ¢ēĒĢ┤ ņŗ£ļĀźņśłĒøäĻ░Ć ļ¦żņÜ░ ņóŗņ¦Ć ņĢŖņ£╝ļ®░, ņ¢æņĢłņ£╝ļĪ£ ņ╣©ļ▓öĒĢĀ Ļ░ĆļŖźņä▒ņØ┤ ņ׳ņ¢┤ ņĀĢĒÖĢĒĢśĻ│Ā ļ╣ĀļźĖ ņ¦äļŗ©Ļ│╝ ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢśļŗż.
ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ ĒÖśņ×ÉņØś ļīĆļČĆļČäņØĆ ĒżļÅäļ¦ēņØś ņŚ╝ņ”ØņØä ļÅÖļ░śĒĢśņ¦Ćļ¦ī, ņĢłņÖĆņŚ╝ņ”ØņØś ņ”ØņāüņØä ļÅÖļ░śĒĢ£ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņØś ņ”ØļĪĆļŖö ĻĄŁļé┤ņŚÉ ņĢäņ¦ü ļ│┤Ļ│ĀļÉ£ ļ░ö ņŚåņ£╝ļ®░, ĒĢ┤ņÖĖņŚÉņä£ ļō£ļ¼╝Ļ▓ī ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż. ļ│Ė ļģ╝ļ¼ĖņŚÉņä£ ņĀ£ņŗ£ļÉ£ ņé¼ļĪĆļŖö 33ņäĖ ņŚ¼ņä▒ņ£╝ļĪ£, ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņÖĆ ņĢłņÖĆņŚ╝ņ”ØņØ┤ ĒĢ©Ļ╗ś ļÅÖļ░śļÉ£, ņĢäņ¦üĻ╣īņ¦Ć ĻĄŁļé┤ņŚÉņä£ļŖö ļ│┤Ļ│ĀļÉ£ ņĀüņØ┤ ņŚåļŖö ļō£ļ¼Ė ņ×äņāü Ļ▓ĮĻ│╝ļź╝ ļ│┤ņŚ¼ ņØ┤ļź╝ ļ│┤Ļ│ĀĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ņ”ØļĪĆļ│┤Ļ│Ā
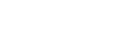
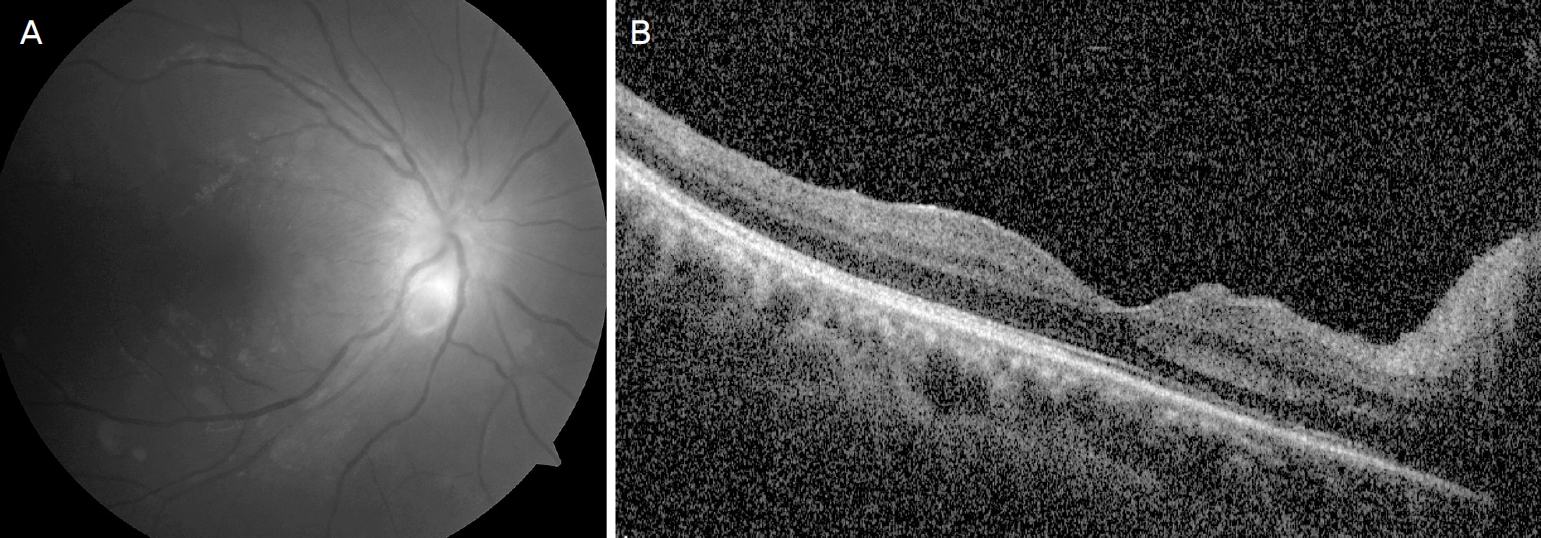
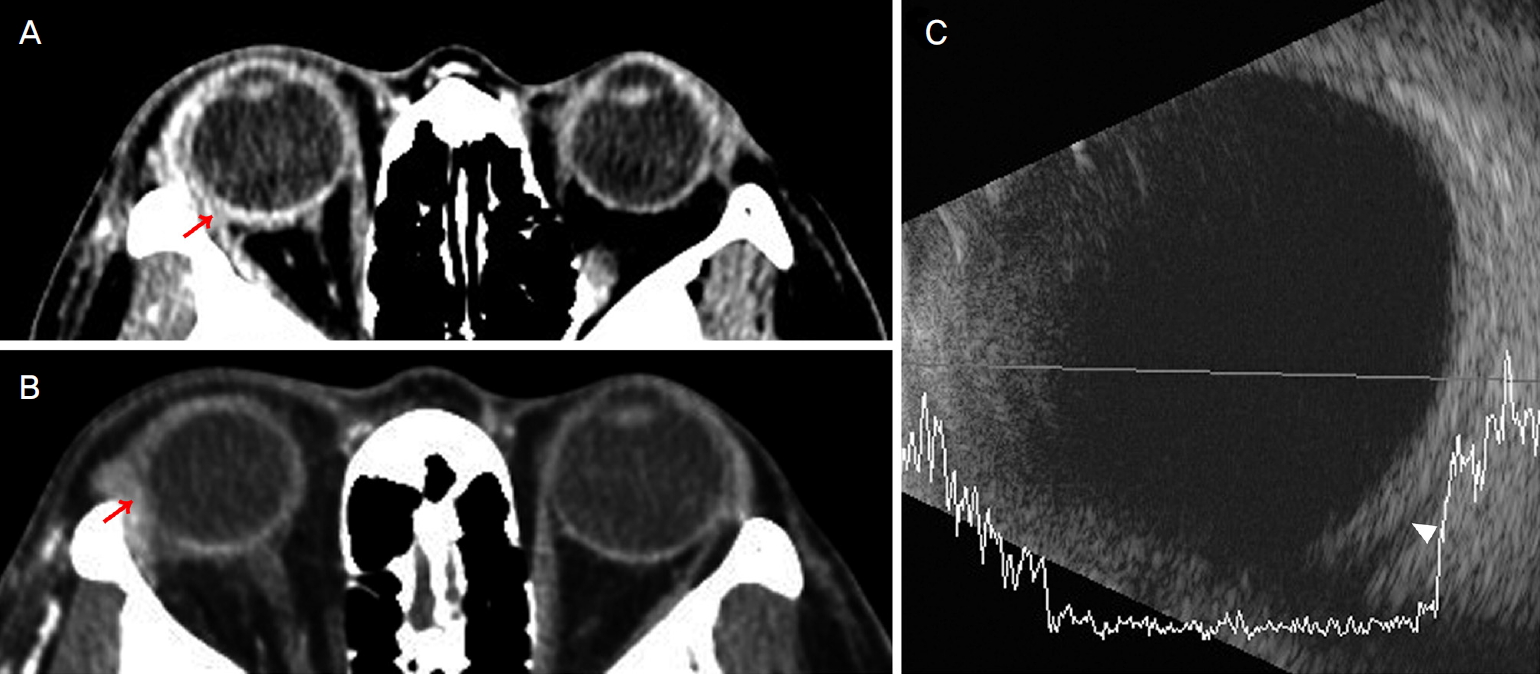
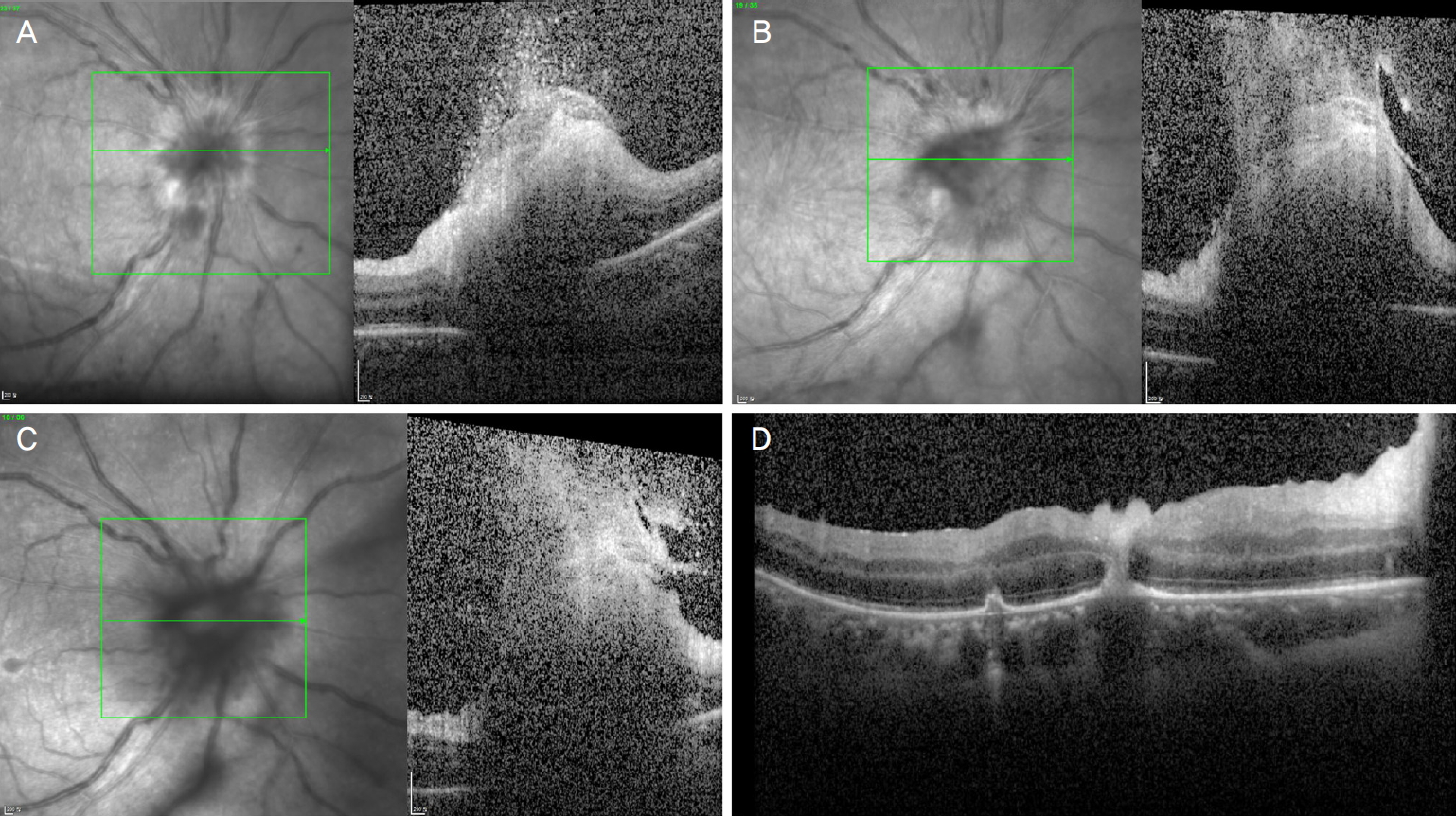
33ņäĖ ņŚ¼ņ×ÉĻ░Ć ļé┤ņøÉ 3ņØ╝ ņĀäļČĆĒä░ ņÜ░ņĢł ņČ®Ēśł, Ļ▓░ļ¦ēļČĆņóģ ļ░Å ĒåĄņ”ØņØä ņŻ╝ņåīļĪ£ ļ│ĖņøÉ ļé┤ņøÉĒĢśņśĆļŗż. 5ļģä ņĀä ņ¢æņĢł ļØ╝ņŗØņłśņłĀ Ļ│╝Ļ▒░ļĀź ņÖĖ ņĀäņŗĀņ¦łĒÖś ļ░Å ņłśņłĀļĀźņØĆ ņŚåņŚłļŗż. ļ│ĖņøÉ ņ┤łņ¦ä ļŗ╣ņŗ£ ļéśņĢłņŗ£ļĀź ņÜ░ņĢł 1.0, ņóīņĢł 1.0ņØ┤ņŚłņ£╝ļ®░, ņĢłņĢĢņØĆ ņÜ░ņĢł 20 mmHg, ņóīņĢł 10 mmHgņśĆļŗż. ņäĖĻĘ╣ļō▒Ēśäļ»ĖĻ▓ĮĻ▓Ćņé¼ņāü ņÜ░ņĢł Ļ▓░ļ¦ēļČĆņóģĻ│╝ ņČ®Ēśł, Standardization of Uveitis Nomenclature ĻĖ░ņżĆņ£╝ļĪ£ ņĀäļ░® ļé┤ ņŚ╝ņ”ØņäĖĒżĻ░Ć 2+ļĪ£ Ļ┤Ćņ░░ļÉśņŚłļŗż. ņĢłņĀĆĻ▓Ćņé¼ņāü ņÜ░ņĢł ņŗ£ņŗĀĻ▓Įņ£ĀļæÉļČĆņóģ ņåīĻ▓¼ ļ░Å ņ£Āļ”¼ņ▓┤ ļé┤ ņŚ╝ņ”ØņäĖĒż ņåīĻ▓¼ņØ┤ ņ׳ņŚłņ£╝ļéś ļ╣øĻ░äņäŁļŗ©ņĖĄņ┤¼ņśü(optical coherence tomography)ņŚÉņä£ ĒÖ®ļ░śļČĆ ņ╣©ļ▓ö ļ░Å, ĒśłĻ┤ĆņŚ╝ņØĆ ļ░£Ļ▓¼ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 1). ņé░ļÅÖ Ēøä ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēņŚÉ ļīĆĒĢ£ ĒÅēĻ░ĆļŖö ņØ┤ļŻ©ņ¢┤ņ¦Ćņ¦Ć ņĢŖņĢśņ£╝ļ®░, ĒżļÅäļ¦ēņŚ╝ Ļ░ĆļŖźņä▒ĒĢś 1.5% levofloxacin (Cravit┬«, Santen Pharmaceutical Co., Ltd., Osaka, Japan), 0.5% loteprednol etabonate (Lotemax┬«, Bausch & Lomb, Tampa, FL, USA)ņØä Ļ░üĻ░ü ĒĢśļŻ© 4ļ▓łņö® ņĀÉņĢłĒĢśĻ▓ī ĒĢśņśĆļŗż. ņ╣śļŻī ņŗ£Ē¢ē ļŗżņØīļéĀ ĒÖśņ×ÉļŖö ņŗ£ļĀźņĀĆĒĢś ļ░Å ļłłĻ║╝ĒÆĆļČĆņóģņØä ĒśĖņåīĒĢśņŚ¼ ņ×¼ļé┤ņøÉĒĢśņśĆļŗż. ņÜ░ņĢł ņŗ£ļĀź 0.7ļĪ£ Ļ░ÉņåīĒĢśņśĆņ£╝ļ®░, ņÜ░ņĢł ņĢłĻĄ¼ļÅīņČ£ 0.5 mm ļ░Å ņÜ░ņĢł ļé┤ņĀäĻ│╝ ņāüĒĢśņĀäņØś ņĀ£ĒĢ£ņØ┤ ļ░£ņāØĒĢśņśĆļŗż(Fig. 2A). ļśÉĒĢ£, Ļ░üļ¦ē Ēøäļ®┤ ņ╣©ņ░®ļ¼╝ņØ┤ ĒÖĢņØĖļÉśņŚłņ£╝ļ®░, ņĀäļ░® ļé┤ ņŚ╝ņ”ØņäĖĒżļŖö 4+ļĪ£ ņ”ØĻ░ĆĒĢ£ ņåīĻ▓¼ņØ┤ņŚłļŗż. ņĢłņÖĆņŚ╝ņ”ØņØś Ļ░Éļ│äņØä ņ£äĒĢ┤ ņĀäņé░ĒÖöļŗ©ņĖĄņ┤¼ņśü(computed tomography, CT) ņ┤¼ņśü ļ░Å ĒśłņĢĪĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. CTņāüņŚÉņä£ ņÜ░ņĢł ĒøäĻ│Ąļ¦ēņØś ņĪ░ņśüņ”ØĻ░ĢņØ┤ ĒÖĢņØĖļÉśņŚłņ£╝ļ®░(Fig. 3A), ņ┤łņØīĒīīĻ▓Ć ņé¼ņāüņŚÉņä£ļÅä ĒøäĻ│Ąļ¦ēņØ┤ ļæÉĻ║╝ņøīņ¦ä Ļ▓āņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż(Fig. 3B). CT ņ┤¼ņśü Ēøä, ņä▒ĒśĢņĢłĻ│╝ņÖĆ ņŗĀĻ▓ĮņĢłĻ│╝ Ēśæņ¦äņØä ņ¦äĒ¢ēĒĢśņśĆņ£╝ļ®░, ņĢłņÖĆņŚ╝ņ”ØņØä ļÅÖļ░śĒĢ£ 2ņ░©ņä▒ ĒøäĻ│Ąļ¦ēņŚ╝, ĒżļÅäļ¦ēņŚ╝ ņØśņŗ¼ ņåīĻ▓¼ņ£╝ļĪ£ ņ×ģņøÉĒĢśņŚ¼ Ļ│ĀņÜ®ļ¤ē ņŖżĒģīļĪ£ņØ┤ļō£ ņ╣śļŻī(Methylprednisolone 250 mg qid)ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ĒśłņĢĪĻ▓Ćņé¼ Ļ▓░Ļ│╝ņāü, C-ļ░śņØæņä▒ ļŗ©ļ░▒ņ¦ł(C-reactive protein) 11.9 mg/dL, ņĀüĒśłĻĄ¼ ņ╣©Ļ░Ģ ņåŹļÅä(erythrocyte sedimentation rate)ļŖö 21.0 mm/hrļĪ£ Ļ░üĻ░ü ņ”ØĻ░ĆĒĢ£ Ļ▓āņØĆ ļŗ╣ņØ╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłņ£╝ļ®░, ņČöĒøä Ļ▓░Ļ│╝Ļ░Ć ĒÖĢņØĖļÉ£ Ēśłņ▓ŁĻ▓Ćņé¼ļĪ£ļŖö HSV immunoglobulin G (IgG) ņ¢æņä▒, HSV IgM equivocal, ļźśļ¦łĒŗ░ņŖż ņØĖņ×É(rheumatoid factor) ņ”ØĻ░Ć, Human Leucocyte Antigen-B51 ņ¢æņä▒, anti-cardiolipin IgG ņĢĮņ¢æņä▒ ņåīĻ▓¼ņ£╝ļĪ£ ņĀĢņāü ļ▓öņ£äļź╝ ļ▓Śņ¢┤ļé¼ņ£╝ļ®░, HSV IgM, syphilis, ņØĖĒä░ĒÄśļĪĀĻ░Éļ¦ł ļČäļ╣äĻ▓Ćņé¼(interferon gamma release assay), toxoplasma IgG/IgM, toxocariasis IgG ļ¬©ļæÉ ņØīņä▒ņØ┤ņŚłļŗż. ĒĢŁĒĢĄĒĢŁņ▓┤(antinuclear antibody)ņÖĆ anti-DNAļÅä ņĀĢņāü ņåīĻ▓¼ņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż. Ļ│ĀņÜ®ļ¤ē ņŖżĒģīļĪ£ņØ┤ļō£ ņ╣śļŻī 1ņØ╝ņ¦Ė(ļé┤ņøÉ 4ņØ╝ņ¦Ė) ļÉśļŖö ļéĀ, ņÜ░ņĢł ļéśņĢł ņŗ£ļĀź 0.6, ņĢłņĢĢ 8 mmHgņ£╝ļĪ£ ĒÖĢņØĖļÉśņŚłņ£╝ļ®░, ļłłĻ║╝ĒÆĆ ļČĆņóģ, Ļ▓░ļ¦ēļČĆņóģ, ņĢłĻĄ¼ ĒåĄņ”ØņØĆ ĒśĖņĀäņØä ļ│┤ņśĆņ£╝ļéś(Fig. 2B), ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēņŚÉ ĒÖ®ļ░▒ņāē ļ░śņĀÉņØś Ļ┤┤ņé¼ ņåīĻ▓¼ ļ░Å ļ¦Øļ¦ēņČ£Ēśł, ĒśłĻ┤ĆņŚ╝ ņåīĻ▓¼(Fig. 4A)ņØ┤ ļ░£Ļ▓¼ļÉśņŚłņ£╝ļ®░, ĒöīļŻ©ņśżļĀłņŗĀ ĒśĢĻ┤æ ņĢłņĀĆņ┤¼ņśü(fluorescein angiography)ņØä ņŗ£Ē¢ēĒĢ£ Ļ▓░Ļ│╝ ņŗ£ņŗĀĻ▓ĮņŚ╝Ļ│╝ ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēņØś ĒśłĻ┤ĆņŚ╝ņØ┤ ĒÖĢņØĖļÉśņŚłļŗż(Fig. 4B). ņØ┤ļź╝ ļ░öĒāĢņ£╝ļĪ£ ņ×äņāüņĀüņ£╝ļĪ£ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ļĪ£ ņ¦äļŗ©ĒĢśĻ│Ā, ļ░öņØ┤ļ¤¼ņŖż ĒÖĢņØĖņØä ņ£äĒĢ┤ ņĀäļ░®ņ▓£ņ×Éļź╝ ĒåĄĒĢ┤ ņĢłĻĄ¼ ļ░®ņłśļź╝ ņ¢╗ņ¢┤ ņżæĒĢ®ĒÜ©ņåīņŚ░ņćäļ░śņØæ(polymerase chain reaction, PCR)Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, ņŖżĒģīļĪ£ņØ┤ļō£ ņĀĢļ¦źņŻ╝ņé¼ļŖö acyclovir 650 mg tid ņĀĢļ¦źņŻ╝ņé¼ļĪ£ ļ│ĆĻ▓ĮĒĢśņśĆļŗż. ņĀÉņĢłņĢĪ Moxifloxacin (Vigamox┬«, Alcon, Fort Worth, TX, USA) ĒĢśļŻ© 4ļ▓ł ņĀÉņĢł, 1% Atropine (Atropine┬«, Alcon) ĒĢśļŻ© 3ļ▓ł ņĀÉņĢłĒĢśļÅäļĪØ ĒĢśņśĆņ£╝ļ®░, aspirin 500 mg ĒĢśļŻ© ĒĢ£ ļ▓ł ļ│ĄņÜ®ĒĢśļÅäļĪØ ĒĢśņśĆņØīņŚÉļÅä ļé┤ņøÉ 5ņØ╝ņ¦Ė ļÉśļŖö ļéĀ, ņĢłĻĄ¼ ņČ®Ēśł ļ░Å ļČĆņóģņØĆ ĒśĖņĀäļÉśņŚłņ£╝ļéś(Fig. 2C), ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ ļ│æļ│ĆņØ┤ ĒÖĢņןļÉśļŖö Ļ▓āņØ┤ ĒÖĢņØĖļÉśņŚłļŗż(Fig. 4C). 6ņØ╝ņ¦Ė ļÉśļŖö ļéĀ, ļéśņĢłņŗ£ļĀź 0.1ļĪ£ ĒÖĢņØĖļÉśņŚłņ£╝ļ®░, ļ│æļ│ĆņØś ņ¦ĆņåŹņĀüņØĖ ĒÖĢņןņ£╝ļĪ£(Fig. 4D) ļ│æļ│Ć ņŻ╝ņ£äņŚÉ ņןļ▓ĮļĀłņØ┤ņĀĆņłĀņØä ņŗ£Ē¢ēĒĢśņśĆņ£╝ļ®░, foscarnet (2.4 mg/0.1 mL)ņØä ņ£Āļ”¼ņ▓┤Ļ░Ģļé┤ ņŻ╝ņé¼ļĪ£ ņŗ£Ē¢ēĒĢśņśĆļŗż. 9ņØ╝ņ¦Ė ļÉśļŖö ļéĀ, ņÜ░ņĢł ņŗ£ļĀź 0.15ļĪ£ ĒÖĢņØĖļÉśņŚłņ£╝ļ®░, ļæÉ ļ▓łņ¦Ė foscarnet (2.4 mg/0.1 mL)ņØä ņ£Āļ”¼ņ▓┤Ļ░Ģļé┤ ņŻ╝ņé¼ļĪ£ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņØ┤Ēøä, ņĀäļ░® ņ▓£ņ×ÉņŚÉņä£ ņŗ£Ē¢ēĒĢ£ PCR Ļ▓Ćņé¼ Ļ▓░Ļ│╝ HSV-2ņØ┤ Ļ▓ĆņČ£ļÉśņŚłļŗż. ņ╣śļŻī 2ņŻ╝ņØ╝ņ¦Ė, ņÜ░ņĢł ļéśņĢłņŗ£ļĀź Ļ┤æĻ░ü ļ¼┤ ņāüĒā£ļĪ£, ņĢłņĀĆĻ▓Ćņé¼ņāü ņŗ£ņŗĀĻ▓ĮļČĆņóģņØ┤ Ļ░ÉņåīĒĢśĻ│Ā, ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēĻ┤┤ņé¼ ļ│æļ│ĆņØĆ ļŹö ĒÖĢņןļÉśņ¦Ć ņĢŖĻ│Ā ņĢłņĀĢņĀüņØĖ ņāüĒā£ļĪ£ ņ£Āņ¦ĆļÉśņŚłļŗż(Fig. 3E). ņØ┤ņŚÉ acyclovir ņĀĢļ¦źņŻ╝ņé¼ļŖö ņ┤Ø 2ņŻ╝Ļ░ä ņé¼ņÜ® Ēøä ņżæņ¦ĆĒĢśņśĆĻ│Ā, prednisolone 1 mg/kg Ļ▓ĮĻĄ¼ ļ│ĄņÜ® ļ░Å valacyclovir 3 gņØä ĒĢśļŻ© 3ĒÜīļĪ£ ļéśļłäņ¢┤ 3ļŗ¼Ļ░ä ļ│ĄņÜ®, aspirin 500 mgņØĆ 1ņŻ╝ ļÅÖņĢł ļ│ĄņÜ®ĒĢśļÅäļĪØ ĒĢśņśĆļŗż. Ēć┤ņøÉ 3ļŗ¼ Ēøä, ņĀäļ░® ļé┤ ņŚ╝ņ”ØņäĖĒżļŖö 2+ļĪ£ ņżäņ¢┤ļōżņŚłņ£╝ļ®░, ņ£Āļ”¼ņ▓┤Ēś╝ĒāüņØĆ ņ׳ņ£╝ļéś ļ│æļ│ĆņØś ĒÖĢņןņØĆ ņŚåņŚłļŗż(Fig. 4F). ĒĢśņ¦Ćļ¦ī ņ£Āļ”¼ņ▓┤Ēś╝Ēāü, ļ¦īņä▒ņĀüņØĖ ņŗ£ņŗĀĻ▓ĮļČĆņóģ ļ░Å ĒŚłĒśłņä▒ ļ│ĆĒÖö, ĻĘĖļ”¼Ļ│Ā ļ¦īņä▒ ņŚ╝ņ”ØņŚÉ ņØśĒĢ£ ĒÖ®ļ░śļČĆņØś ļ│Ćņä▒ ļ░Å ļ¦īņä▒ ĒÖ®ļ░śļČĆņóģņ£╝ļĪ£(Fig. 5) ņÜ░ņĢł ĻĄÉņĀĢņŗ£ļĀźņØĆ ņĢłņĀä ņłśļÅÖņ£╝ļĪ£ ņĀĆĒĢśļÉ£ ņāüĒā£Ļ░Ć ņ¦ĆņåŹļÉśņŚłļŗż. ņóīņĢłņØĆ ņāłļĪ£ņÜ┤ ļ│æļ│ĆņØś ļ░£ņāØ ņŚåņØ┤ ņĢłņĀĢņĀüņ£╝ļĪ£ ņ£Āņ¦ĆļÉśĻ│Ā ņ׳ļŗż.
Ļ│Ā ņ░░
1994ļģä American Uveitis SocietyņŚÉņä£ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ļŖö ņ×äņāüņĀüņ£╝ļĪ£ ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēņŚÉ Ļ▓ĮĻ│äĻ░Ć ļ¬ģĒÖĢĒĢ£ ĒĢśļéś ņØ┤ņāüņØś Ļ┤┤ņé¼ ļ│æļ│ĆņØ┤ ņ׳ņ£╝ļ®┤ņä£, ļ│æļ│ĆņØĆ ņŻ╝ļ│Ćņ£╝ļĪ£ ĒÖĢņןĒĢśļ®░, ņŻ╝ļĪ£ ļÅÖļ¦źņØä ņ╣©ļ▓öĒĢśļŖö ĒÅÉņćäĒśłĻ┤Ćļ│æņ”Ø, ņĀäļ░®Ļ│╝ ņ£Āļ”¼ņ▓┤ņŚ╝ņ”ØņØä ļÅÖļ░śĒĢśĻ│Ā, ĒĢŁļ░öņØ┤ļ¤¼ņŖż ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņØä Ļ▓ĮņÜ░ ĻĖēņåŹļÅäļĪ£ ņ¦äĒ¢ēļÉśļŖö ĒŖ╣ņ¦ĢņØä Ļ░Ćņ¦äļŗżĻ│Ā ņĀĢņØśĒĢśņśĆļŗż[4]. ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ĒŖ╣ņØ┤ ļ│æļĀźņØ┤ ņŚåļŹś 33ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉĻ░Ć Ļ░æņ×æņŖżļ¤░ ņĢłĻĄ¼ĒåĄņ”Ø, Ļ▓░ļ¦ē ņČ®ĒśłĻ│╝ ļČĆņóģņ£╝ļĪ£ ļé┤ņøÉĒĢśņŚ¼ ņĢłņĀĆĻ▓Ćņé¼ņāü ņŗ£ņŗĀĻ▓Įņ£ĀļæÉļČĆņóģ ņåīĻ▓¼Ļ│╝ ņśüņāü Ļ▓Ćņé¼ņāü ņĢłņÖĆņŚ╝ņ”Ø ļ░Å ĒżļÅäļ¦ēņŚ╝ ņåīĻ▓¼ņØ┤ ņ׳ņŚłņ£╝ļ®░, ņØ┤Ēøä ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēĻ┤┤ņé¼, ņ£Āļ”¼ņ▓┤ņŚ╝ņ”Ø ļō▒ņØ┤ ļ░£Ļ▓¼ļÉśņ¢┤ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ļź╝ ņ¦äļŗ©ļ░øņØĆ Ļ▓ĮņÜ░ļź╝ ņé┤ĒÄ┤ļ│┤ņĢśļŗż. ĒÖśņ×ÉļŖö ņĀäļ░®ņ▓£ņ×É PCR Ļ▓Ćņé¼ņāü HSV-2Ļ░Ć Ļ▓ĆņČ£ļÉśņŚłņ£╝ļ®░, ĒĢŁļ░öņØ┤ļ¤¼ņŖżņĀ£ ņŻ╝ņé¼ ņ╣śļŻī 2ņŻ╝ Ļ░ä ņ¦ĆņåŹĒĢ£ Ēøä Ļ▓ĮĻĄ¼ ĒĢŁļ░öņØ┤ļ¤¼ņŖżņĀ£ļź╝ 3ļŗ¼ Ļ░ä ņé¼ņÜ®ĒĢśņśĆļŗż.
ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņÖĆ ņĢłņÖĆņŚ╝ņ”ØņØ┤ ļÅÖļ░śļÉ£ Ļ▓ĮņÜ░ļŖö ĒĢ┤ņÖĖņŚÉņä£ ļ¦żņÜ░ ļō£ļ¼╝Ļ▓ī ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ£╝ļ®░ ĻĄŁļé┤ņŚÉņä£ļŖö ņĢäņ¦üĻ╣īņ¦Ć ļ│┤Ļ│ĀļÉ£ ņĀüņØ┤ ņŚåļŗż. Ēśäņ×¼Ļ╣īņ¦Ć ĒĢ┤ņÖĖņŚÉņä£ ļ░£Ēæ£ļÉ£ ņé¼ļĪĆļōżņØä ņé┤ĒÄ┤ļ│┤ļ®┤, 2000ļģä 34ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉņŚÉņä£ HSV-1ņŚÉ ņØśĒĢ┤ ņĢłĻĄ¼ļÅīņČ£ņØä ļÅÖļ░śĒĢ£ ņĢłņÖĆņŚ╝ņ”ØĻ│╝ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼Ļ░Ć ļÅÖļ░śļÉ£ ņé¼ļĪĆĻ░Ć ņ׳ņ£╝ļ®░[5], 2003ļģäņŚÉļÅä ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ ņ¦äļŗ© ļŗ╣ņŗ£ ņĢłņÖĆņŚ╝ņ”ØņØ┤ ļÅÖļ░śļÉ£ 30ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉņØś ņé¼ļĪĆĻ░Ć ļ│┤Ļ│ĀļÉśņŚłņ£╝ļ®░ ņĀäļ░® ņ▓£ņ×É PCRņŚÉņä£ HSV-1ņØ┤ Ļ▓ĆņČ£ļÉśņŚłļŗż[6]. ņÖĖņĢłĻĘ╝ņŚ╝ņØä ļÅÖļ░śĒĢ£ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņØś ņé¼ļĪĆņŚÉņä£ļÅä ņĀäļ░®ņ▓£ņ×É PCRņŚÉņä£ HSV-2Ļ░Ć Ļ▓ĆņČ£ļÉ£ 49ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉņÖĆ ļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ▓ĆņČ£ļÉśņ¦Ć ņĢŖņĢśļŹś 81ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉņØś ņé¼ļĪĆĻ░Ć ņåīĻ░£ļÉśņŚłļŗż[7,8]. 2019ļģäņŚÉļŖö 73ņäĖ ļé©ņ×É ĒÖśņ×ÉņÖĆ 18ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉņØś ņé¼ļĪĆ[9]Ļ░Ć ļ░£Ēæ£ļÉśņŚłņ£╝ļ®░, Ļ░üĻ░ü ņĀäļ░®ņ▓£ņ×É PCR Ļ▓Ćņé¼ņŚÉņä£ HSV-2, HSV-1ņØ┤ Ļ▓ĆņČ£ļÉśņŚłļŗż. ļ│Ė ņ”ØļĪĆļź╝ ĒżĒĢ©ĒĢśņŚ¼ ļ│┤Ļ│ĀļÉ£ 8ļ¬ģņØś ĒÖśņ×ÉļōżņØś Ļ▓ĮņÜ░ļź╝ ņĀĢļ”¼ĒĢ┤ļ│┤ļ®┤, ņĀäļ░®ņ▓£ņ×É PCRņŚÉņä£ 8ļ¬ģ ņżæ HSV-1, HSV-2 Ļ░üĻ░ü 3ļ¬ģņö® Ļ▓ĆņČ£ļÉśņŚłņ£╝ļ®░, ļŗżļźĖ 2ļ¬ģņŚÉņä£ļŖö ļ░öņØ┤ļ¤¼ņŖżĻ░Ć Ļ▓ĆņČ£ļÉśņ¦Ć ņĢŖņĢśļŗż.
ņØ┤ņ▓śļ¤╝ HSVņŚÉ ņØśĒĢ┤ ņĢłļé┤ņŚ╝ņ”ØĻ│╝ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼Ļ░Ć ļÅÖņŗ£ņŚÉ ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░ļŖö ļ¦żņÜ░ ļō£ļ¼╝Ļ▓ī ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ¢┤ ņĢäņ¦ü ņøÉņØĖņØ┤ ļ¬ģĒÖĢĒĢśĻ▓ī ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśļŗż. Ēśäņ×¼ ņØ╝ļČĆ ņŚ░ĻĄ¼ņŚÉņä£ ņĀ£ĻĖ░ļÉśļŖö Ļ░ĆļŖźņä▒ņ£╝ļĪ£ļŖö ņĢłņÖĆ ņŻ╝ņ£äņŚÉ ņ£äņ╣śĒĢ£ ņä¼ļ¬©ņŗĀĻ▓ĮņĀłņØś ĒŚżļź┤ĒÄśņŖż ļ░öņØ┤ļ¤¼ņŖż ņ×¼ĒÖ£ņä▒ņ£╝ļĪ£, ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņÖĆ ļÅÖņŗ£ņŚÉ ņĢłņÖĆņŚ╝ņ”Ø ļ░śņØæņØä ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŗżĻ│Ā ņĀ£ņŗ£ĒĢśĻ│Ā ņ׳ļŗż[10,11 ].
ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ļŖö ņĀäņŗĀ ļ░Å ņ£Āļ”¼ņ▓┤Ļ░Ģ ļé┤ ĒĢŁļ░öņØ┤ļ¤¼ņŖżņĀ£ ņ╣śļŻī, ņŖżĒģīļĪ£ņØ┤ļō£ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢ£ļŗż. ņØ┤ĒÖśļÉ£ ļłłņØś ņĄ£ņóģ ņŗ£ļĀźņØĆ ļ¦Øļ¦ēļ░Ģļ”¼, ĒŚłĒśłņŗ£ņŗĀĻ▓Į ļ░Å ļ¦Øļ¦ēļ│æņ”Ø, ļ¦īņä▒ ņ£Āļ”¼ņ▓┤ņŚ╝ ļ░Å ĒÖ®ļ░śļČĆņóģ, ļ¦Øļ¦ēņĢ×ļ¦ē ļō▒ņŚÉ ņØśĒĢ┤ ņĢĮ ņĀłļ░śņØś ĒÖśņ×ÉņŚÉņä£ ņ╣śļŻīņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā 0.1 ņØ┤ĒĢśļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż. ĻĘĖņżæ ļ¦Øļ¦ēļ░Ģļ”¼ņØś ļ░£ņāØņØ┤ 20%ņŚÉņä£ 73%Ļ╣īņ¦Ć ļ│┤Ļ│ĀļÉśņ¢┤ ņŗ£ļĀźņĀĆĒĢśņØś ņŻ╝ ņøÉņØĖņØä ņ░©ņ¦ĆĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņśłļ░®ņĀü ņןļ▓Į ļĀłņØ┤ņĀĆļź╝ ņŗ£Ē¢ēĒĢśĻĖ░ļÅä ĒĢśļéś, ļ¦Øļ¦ēļ░Ģļ”¼ņØś ņśłļ░® ĒÜ©Ļ│╝Ļ░Ć ļ¬ģĒÖĢĒĢśĻ▓ī ļ░ØĒśĆņ¦Ćņ¦ĆļŖö ņĢŖņĢśļŗż[12,13]. ļ│Ė ņ╝ĆņØ┤ņŖżņØś Ļ▓ĮņÜ░, ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņØś ņĀüĻĘ╣ņĀüņØĖ ņ╣śļŻīņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ļ¦īņä▒ņĀüņØĖ ņ£Āļ”¼ņ▓┤ņŚ╝ņ”Ø, ņŗ£ņŗĀĻ▓ĮņØś ĒŚłĒśłņä▒ ļ│ĆĒÖö ļ░Å ļ¦īņä▒ļČĆņóģ, ĻĘĖļ”¼Ļ│Ā ĒÖ®ļ░śļČĆņØś ļ│Ćņä▒ ļ░Å ļ¦īņä▒ļČĆņóģņ£╝ļĪ£ ņØĖĒĢ┤ ņĄ£ņóģ ņŗ£ļĀźņśłĒøäļŖö ļ¦żņÜ░ ļČłļ¤ēĒĢśņśĆļŗż.
ļ│Ė ņ”ØļĪĆļŖö ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼Ļ░Ć ļ░£ņāØĒĢśļ®┤ņä£ ņĢłņÖĆņŚ╝ņ”ØņØ┤ ļÅÖņŗ£ņŚÉ ļ░£ļ│æĒĢ£ ļō£ļ¼Ė ņ”ØļĪĆļĪ£, ņ┤łĻĖ░ Ļ▓Ćņé¼ ļ░Å ņ╣śļŻīĻ░Ć ņĢłņÖĆņŚ╝ņ”ØņŚÉ ļīĆĒĢ£ ĒÅēĻ░Ć ļ░Å ņ╣śļŻīņŚÉ ņ¦æņżæļÉśņ¢┤ ļ¦Øļ¦ē ņŻ╝ļ│ĆļČĆņÖĆ Ļ░ÖņØĆ ņĢłĻĄ¼ ļé┤ļČĆņØś ĒÅēĻ░ĆĻ░Ć ņ┤łĻĖ░ņŚÉ ņĀüņĀłĒĢśĻ▓ī ņØ┤ļŻ©ņ¢┤ņ¦Ćņ¦Ć ļ¬╗ĒĢśņŚ¼ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼Ļ░Ć ļŖ”Ļ▓ī ņ¦äļŗ©ļÉśņ¢┤ ņ╣śļŻīĻ░Ć ļŖ”Ļ▓ī ņŗ£Ē¢ēļÉ£ ņ”ØļĪĆņØ┤ļŗż. ļö░ļØ╝ņä£ ņĢłņÖĆņŚ╝ņ”ØĻ│╝ ĒżļÅäļ¦ēņŚ╝ņØ┤ ļÅÖļ░śļÉ£ ĒÖśņ×ÉĻ░Ć ļé┤ņøÉĒĢśņśĆņØä Ļ▓ĮņÜ░, ņ£Āņ£Īņóģ(sarcoidosis), Ļ▓░ĒĢĄ(tuberculosis), ļ¦żļÅģ(syphilis) ļō▒ņØä Ļ░Ćņן ļ©╝ņĀĆ ņØśņŗ¼ĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī, ļ░śļō£ņŗ£ ņŻ╝ļ│ĆļČĆ ļ¦Øļ¦ēņØś ĒÖĢņØĖņØä ņ¦äĒ¢ēĒĢśņŚ¼ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņØś ņ¦äļŗ©ņØ┤ ļŖ”ņ¢┤ņ¦ĆļŖö ņØ╝ņØ┤ ļ░£ņāØĒĢśņ¦Ć ņĢŖļÅäļĪØ ĒĢ┤ņĢ╝ ĒĢ£ļŗż.
Ļ▓░ļĪĀņĀüņ£╝ļĪ£ ĒżļÅäļ¦ēņŚ╝Ļ│╝ ņĢłņÖĆņŚ╝ņ”ØņØ┤ ļÅÖļ░śļÉśļŖö Ļ▓ĮņÜ░ ņ×äņāüņØśļŖö ļ░śļō£ņŗ£ ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ Ļ░ĆļŖźņä▒ņØä Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż. ĻĖēņä▒ļ¦Øļ¦ēĻ┤┤ņé¼ņÖĆ Ļ┤ĆļĀ©ļÉ£ ņŗ¼Ļ░üĒĢ£ ĒĢ®ļ│æņ”ØņØä ņżäņØ┤ļĀżļ®┤ PCRļĪ£ ĒÖĢņØĖļÉśĻĖ░ ņĀä acyclovirļź╝ ņé¼ņÜ®ĒĢ£ ņ”ēĻ░üņĀüņØĖ ņ╣śļŻīļź╝ ņ¦Ćņ▓┤ ņŚåņØ┤ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






